User login
Four Fracture Patterns Unique to Pediatric Patients
Case 1
A 2-year-old girl presented to the ED with arm pain. Her mother stated that her daughter was playing with a 5-year-old sibling when she heard the child cry- out in pain and noticed she was holding her right arm by her side, not wanting to move it. Neither child gave a reliable story of the injury.
Nursemaid’s Elbow
Nursemaid’s elbow, also known as pulled elbow, subluxation of the radial head, and most recently annular ligament displacement, is a common injury in children younger than age 6 years. One study estimates that the condition represented about 1% of injury-related ED visits in 2005.1
Patients with nursemaid’s elbow typically present holding the injured arm at their side, slightly flexed and pronated. These patients appear relatively comfortable until moved actively or passively. The classic history of nursemaid’s elbow includes a traction mechanism, with the child being pulled up by one arm or being grabbed by the arm suddenly to keep him or her out of harm’s way.2 Due to the laxity of connective tissues in children of this age, the head of the radius slips out of the annular ligament causing acute pain and decreased function.
Nursemaid’s elbow is usually diagnosed by history and examination alone, with special consideration to the mechanism of injury. There is rarely swelling or bruising.3 Passive flexion and extension at the elbow may be normal, but rotational maneuvers can be painful or fully resisted.
Reduction Techniques
In 2012, Cochrane updated its earlier review on nursemaid’s elbow and in 2013 followed up with an article in Pediatrics in Review.3,4 Each covered research on reduction techniques, summarizing studies comparing supination-flexion (SF) versus hyperpronation (HP) as the initial reduction maneuver. Given that these maneuvers are difficult to camouflage, studies tend to be pseudorandomized with assessment by a nonblinded healthcare provider, decreasing the strength of the studies. In the Cochrane review, four different trials that included 379 children under age 7 years were selected for the review. In all four studies, pronation was found to have the least chance of failed first attempt, the chosen outcome for this meta-analysis. The risk ratio of failure of reduction for pronation was 0.45 (95% confidence interval [CI], 0.28-0.73).
There is some data supporting hyperpronation to be less painful as well; however, the Cochrane reviewers felt there may have been reporting bias.4 Since the time of each of these reviews, another study comprised of 150 children was conducted and also favored similar practice styles, as the hyperpronation maneuver had 95% success rate on first attempt versus 68% first-time success with supination and flexion.5
Complications and Recurrence
In a small study aimed at identifying recurrence rates for nursemaid’s elbow, Teach and Schultzman6 studied 93 children for 1 year after probable or definite diagnosis of nursemaid’s elbow. Of these children, 23.7% had recurrent radial head subluxation. Children younger than age 2 years were found to have a relative risk of 2.6 (95% CI, 1.04-6.30) for one or more recurrences when compared to children older than age 2 years.
While the great majority of children with nursemaid’s elbow do not need referral to an orthopedist, those with two or more occurrences should be considered for referral to a specialist.
Case 2
A 6-year-old boy was presented to the ED by his father, who had placed the boy’s arm in a home-made sling. The child tearfully told the provider that he fell trying to catch himself after tripping over the house pet.
FOOSH Injury
The above case depicts a very common presentation in the ED—the so-called “FOOSH” (fall onto an outstretched hand) injury. This type of injury occurs with such frequency in both adults and children that it is one of the only injury patterns with a commonly used acronym. The bony injuries seen with FOOSH in children, however, have a different pattern than those in adults.
Pediatric fractures are unique due to the difference in the structure of the bones themselves. A child’s bones are more elastic than an adult’s bones, allowing them to bow and bend before they fracture.7 Despite this malleability, pediatric bones have been noted to have a thicker periosteum. For this reason, compression or impact may interrupt the periosteal sleeve, minimally yielding an incomplete interruption of the cortex unilaterally.

One fracture pattern commonly seen in children is the torus fracture. This type of fracture is also referred to as a buckle fracture as the bone cortex on radiographic imaging appears “buckled” as a result of the compressive forces on that side of the bone (Figure 1). Since the bone itself is minimally affected, these fractures are quite stable and not at risk for complications.
In comparison, a greenstick fracture, also unique to the pediatric population, is one in which the cortex shows plastic deformity on the side of the force or impact but is interrupted on the opposite side due to the tension of the impact itself. Greenstick fractures are frequently angulated and may require reduction for anatomic alignment, but long-term complications are typically minimal. These fracture patterns are distinguished from complete fractures (as seen in adults), which are quite unstable and generally require surgical intervention.
Of note, the location of pediatric forearm fractures varies with age as well. Diaphyseal fractures are more common in prepubescent children, whereas the highest incidence of physeal injuries occurs during large growth spurts, particularly throughout adolescence.7
Management
The remodeling potential of pediatric bones also makes management unique. Pediatric orthopedic literature has well-studied acceptable angles and degrees of appropriate displacement based largely on the age of the patient and proximity to a growth plate. Knowledge of these is imperative for definitive care of such fractures but is beyond the scope of this review.
Traditional treatment of pediatric forearm fractures includes immobilization of various types and duration to minimize pain and deformity while producing the best possible outcome. Several recent studies have aimed to determine best practice for the different fracture types with the goal of producing best alignment and return to function while decreasing cost, discomfort, and number of physician visits. Another concern among healthcare providers is the risk of refracture, which in buckle fractures is estimated at approximately 2% with a median time of 8 to 16 weeks after the initial injury.7
A 2010 review by Kennedy et al8 sought to determine if the refracture rate was affected by the technique used to immobilize torus fractures. The five studies used in this review had no reports of refracture in the 443 patients included in analysis, though only one of the studies (Plint et al) followed patients for more than 6 weeks.8,9 In this study, 75 patients were randomized to either a plaster removable splint or full below-elbow cast for 3 weeks; thereafter, they were followed for 6 months, during which time none experienced refracture.9
Another outcome from the same study assessed the ability of the patient to use the affected arm in the recovery period. While those in removable splints scored better during and immediately after cast removal, no differences were present after 1 week. Not surprisingly, families preferred the soft bandages or a removable splint for treatment.
Case 3
A 13-year-old boy presented to the ED with right ankle pain and difficulty bearing weight. He stated that he was playing basketball when he “rolled” his right ankle coming down from a rebound.
Ankle Fractures
Ankle fractures are among the most common acute injuries of the lower extremity in children, accounting for approximately 5% of pediatric fractures and 15% of physeal injuries.10 Ankle fractures also account for up to 40% of all injuries to the skeletally immature athlete.10,11 More specifically, distal fibular physeal fractures are the most common types of pediatric ankle fracture; however, they are associated with a relatively low risk for long-term complications. In contrast, distal tibial physeal fractures are associated with a higher risk for long-term complications.12,13
Presentation and Evaluation
Typically, patients presenting with ankle fractures are too sore to bear weight, and swelling and ecchymosis can be identified anterior to the ankle. In addition, there may be diffuse tenderness throughout the ankle and point tenderness may be induced on the anterolateral aspect of the distal tibia.14 A complete evaluation of the entire lower extremity should be conducted before assuming that the injury is confined to the ankle, especially in children younger than age 5 years and/or who are nonverbal.10 When evaluating an ankle fracture, in general, orthopedic consultation should be obtained for children with neurovascular compromise, open fractures, and/or Salter-Harris III, IV, and V fractures.
The juvenile Tillaux fracture represents a Salter-Harris III physeal injury that involves the anterolateral portion of the tibia. It usually occurs in children between ages 12 and 14 years as they approach skeletal maturity and who have a partially fused tibial physis. The common mechanism of injury is inversion of the ankle with the foot pointed away from the midline (supination with external rotation). This leads to avulsion of the lateral tibial epiphysis that is attached to the anterior inferior tibiofibular ligament. The uninvolved medial portion of the epiphysis is closed.10
Radiographic Imaging

Three radiographic views should be obtained in the evaluation of pediatric ankle injuries as Tillaux fractures or other subtle injuries could be easily missed if only two views are obtained. Interpretation of the radiographs must be correlated with the physical examination.10 The fracture line is usually best seen on a mortise view (Figure 2). Computed tomography (CT) is warranted in cases in which displacement greater than 2 mm is suspected because it better defines fracture displacement and can aid in surgical planning.14 Because of its sensitivity in detecting fractures displaced more than 2 mm, CT is now the preferred imaging modality in the assessment of juvenile Tillaux fractures.15
Definitive Management
There are two important goals when treating children with ankle fractures—achieving a satisfactory reduction and avoiding physeal arrest so as to minimize the risks of angular deformity, early arthrosis, leg-length inequality, and joint stiffness.11 Juvenile Tillaux fractures with greater than 2 mm of displacement require orthopedic consultation for closed or open reduction. Closed reduction is attempted by internally rotating the foot and applying direct pressure over the anterolateral tibia. If necessary, percutaneous pins can be used for stabilization of the reduction. If closed reduction is unsuccessful, open reduction is required. Care must be taken to assure no displacement occurs after casting; this requires weekly X-ray evaluation for the first 2 weeks.12
Patients with nondisplaced Salter-Harris III fractures are treated with long-leg casting for 4 weeks with conversion to a short-leg cast or boot for an additional 4 weeks. Patients should anticipate 8 weeks of nonweight-bearing. The patient is allowed to remove the boot for range-of-motion exercises but must remain nonweight-bearing for the first 2 weeks.14
Case 4
A 3-year-old previously healthy girl presented to the ED with a limp and difficulty bearing weight. Her mother reported that the child was playing in the yard when she caught her foot on a tree root, stumbled, and fell down. Since the incident, the child has been tearful, limping, and refusing to walk.
Tibial Fractures
Tibial fractures are among the most frequent types of orthopedic injuries in young children, with only femur and forearm fractures having a higher incidence of occurrence. Tibial fractures account for up to 15% of long bone fractures in children and adolescents.16,17 The mechanism of injury varies depending on the patient’s age. In young children, the most common cause of injury is from a seemingly minor twisting around a fixed foot or from a minor fall. In older children and adults, high-energy motor vehicle accidents and sports-related injuries are more common causes.
Fractures of the tibial shaft are typically short oblique or transverse fractures of the middle or distal third of the shaft. Thirty percent of tibial shaft fractures are associated with fractures of the fibula.16
Toddler’s Fracture
The term toddler’s fracture refers to a nondisplaced oblique fracture of the tibial shaft without concomitant fibular fracture. It usually results from an indirect rotational or twisting force applied to the foot and lower leg.16-18 More specifically, the term describes a specialized case of spiral fracture of the distal tibia in patients aged 9 months to 3 years, when weight-bearing is just beginning.19,20 Such injuries commonly occur when a toddler stumbles and falls, or attempts to extricate the foot from between the bars of a crib. Often, however, the mechanism is minimal or unknown.18 Of those injuries that are witnessed, most caregivers report a minor twisting mechanism. Most children with toddler’s fracture are younger than age 6 years. Sixty-three of 76 such fractures reported by Dunbar et al17,19 occurred in children younger than 2.5 years of age. Toddler’s fractures occur more often in boys than girls, and in the right leg more often than the left. Most children will give a history of tripping or twisting their ankle.17
Evaluating the Toddler
Toddlers can be challenging patients as they can not relate history and are often uncooperative on examination. A child may present with a limp, diminished movement of the affected limb, or refuse to bear weight without a distinct history of injury. The onset of limping or refusal to bear weight after minor trauma, or without an obvious injury in a young ambulatory child, warrants a detailed examination looking for tenderness over the tibia, along with radiographic evaluation to rule out a toddler’s fracture.
The examination of the patient is rarely impressive as there is little swelling and bruising with most toddlers’ fractures. A complete clinical history is needed, including a detailed description of any observed traumatic event to exclude the existence of other injuries.
When no traumatic event is observed or an inconsistent history is provided, the physician should obtain a detailed social history, including a list of the child’s most recent caregivers and contacts.16 Because of mild clinical symptoms and frequent lack of a history of injury in this patient population, presentation for evaluation may be delayed. In such cases, by the time the extremity is examined, the fracture has begun to heal. This healing phase may be accompanied by periosteal new bone and, in the absence of a history, may erroneously suggest other, more ominous conditions such as osteomylelitis or tumor.17,18
Consideration of Abuse
Although tibial shaft fractures are rarely found in abused children, diagnosis of child abuse must be considered in cases where a tibial fracture is discovered in the nonambulatory child; his or her clinical history is inconsistent with the injury; and/or there are other physical findings suggestive of abuse. Investigation for suspected nonaccidental trauma includes a thorough physical examination, skeletal survey, and evaluation by social services personnel.16
Radiographic Imaging
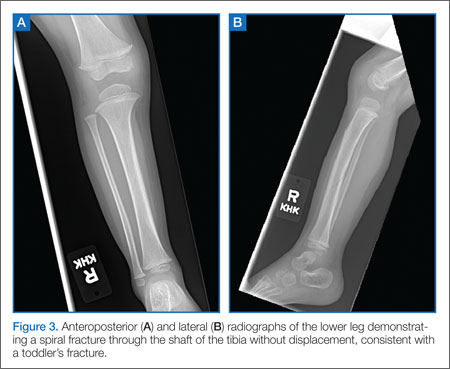
Quality anteroposterior (AP) or lateral radiographs of the affected leg may show a hairline fracture, but these can easily be missed on initial plain films in almost a third of patients.21 An internal oblique view can aid in identifying nondisplaced toddler fractures.17 The AP view is the best view for observing the nondisplaced spiral fracture along the distal tibia (Figure 3).6 Occasionally, a fracture line is not identified on initial plain films and the first evidence of fracture becomes apparent on X-ray when new periosteal bone forms 7 to 10 days after the initial injury.
Definitive Treatment
Children with a classic history for a toddler’s fracture and an inability to bear weight should be immobilized with a long-leg splint or cast—even when X-rays are negative—until a definitive diagnosis can be made. Such fractures usually become visible on X-ray 7 to 10 days after injury as a result of new bone growth.22
When definitive diagnosis of a toddler’s fracture is made on plain radiographs, the child should either be immobilized in a long-leg splint with referral to an orthopedist within 5 to 7 days, or immediately casted.16
Conclusion
Fractures in both children and adults are among the most common injury-related presentations to the ED. Based on the structure and increased elasticity of bone in the pediatric patient, there are several fracture patterns unique to this population. Appropriate evaluation, diagnosis, and management in the ED helps to maximize and ensure long-term function and healing while minimizing trauma to the patient.
Dr McBride is an associate professor of pediatrics and pediatric emergency medicine, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
Dr Sutton is a pediatric resident, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
- Brown D. Emergency department visits for nursemaid’s elbow in the United States, 2005-2006. Orthop Nurs. 2009;28(4):161,162.
- Hardy RH. Pulled elbow. J R Coll Gen Pract. 1978;28(189):224-226.
- Browner EA. Nursemaid’s elbow (annular ligament displacement). Pediatr Rev. 2013;34(8):366,367.
- Krul M, van der Wouden JC,van Suijlekom-Smit LW, Koes BM. Manipulative interventions for reducing pulled elbow in young children. Cochrane Database of Syst Rev. 2012;1:CD007759.
- Gunaydin YK, Katirci Y, Duymaz H, et al. Comparison of success and pain levels of supination-flexion and hyperpronation maneuvers in childhood nursemaid’s elbow cases. Am J Emerg Med. 2013;31(7):1078-1081.
- Teach SJ, Schutzman SA. Prospective study of recurrent radial head subluxation. Arch Pediatr Adolesc Med. 1996;150(2):164-166.
- Dolan M and Waters PM. Fractures and dislocations of the forearm, wrist, and hand. In: Green NE, Swiontkowski MF, eds. Skeletal Trauma in Children. 4th ed. Philadephia, PA: Saunders Elsevier; 2009:159-206.
- Kennedy SA, Slobogean GP, Mulpuri K. Does degree of immobilization influence refracture rate in the forearm buckle fracture? J Pediatr Orthop B. 2010;19(1):77-81.
- Plint AC, Perry JJ, Correll R, Gaboury I, Lawtown L. A randomized, controlled trial of removable splinting versus casting for wrist buckle fractures in children. Pediatrics. 2006;117(3):691-697.
- Kay RM, Matthys GA. Pediatric ankle fractures: evaluation and treatment. J Am Acad Orthop Surg. 2001;9(4):268-278.
- Marsh JS, Daigneault JP. Ankle injuries in the pediatric population. Curr Opin Pediatr. 2000;12(1):52-60
- Cummings RJ. Distal tibial and fibular fractures. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins’ Fractures in Children. 6th ed. Pennsylvania, PA: Lippincott Williams & Wilkins; 2006:1096-1104.
- Boutis K, Willan AR, Babyn P, Narayanan UG, Alman B, Schuh S. A randomized, controlled trial of a removable brace versus casting in children with low-risk ankle fractures. Pediatrics. 2007;119(6):1256-1263.
- Wuerz TH, Gurd DP. Pediatric physeal ankle fracture. J Am Acad Orthop Surg. 2013;21(4):234-244.
- Horn BD, Crisci K, Krug M, Pizzutillo PD, MacEwen GD. Radiologic evaluation of juvenile Tillaux fractures of the distal tibia. J Pediatr Orthop. 2001;21(2):162-164.
- Mashru RP, Herman MJ, Pizzutillo PD. Tibial shaft fractures in children and adolescents. J Am Acad Orthop Surg. 2005;139(5):345-352.
- Heinrich SD, Mooney JF. Fractures of the shaft of the tibia and fibula. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins’ Fractures in Children. 6th ed. Pennsylvania, PA: Lippincott Williams & Wilkins; 2006:1063,1064.
- John SD, Moorthy CS, Swischuk LE. Expanding the concept of the toddler’s fracture. Radiographics. 1997;17(2):367-376.
- Dunbar JS, Owen HF, Nogrady MB, McLeese R. Obscure tibial fracture of infants—the toddlers’ fracture. J Can Assoc Radiol 1964;15:136-144.
- Tenenbein M, Reed MH, Black GB. The toddler’s fracture revisited. Am J Emerg Med. 1990;8(3):208-211.
- Shravat BP, Harrop SN, Kane TP. Toddler’s fracture. J Accid Emerg Med. 1996;13(1):59-61.
- Halsey MF, Finzel KC, Carrion WV, Haralabatos SS, Gruber MA, Meinhard BP. Toddler’s fracture: presumptive diagnosis and treatment. J Pediatr Orthop. 2001;21(2):152-156.
Case 1
A 2-year-old girl presented to the ED with arm pain. Her mother stated that her daughter was playing with a 5-year-old sibling when she heard the child cry- out in pain and noticed she was holding her right arm by her side, not wanting to move it. Neither child gave a reliable story of the injury.
Nursemaid’s Elbow
Nursemaid’s elbow, also known as pulled elbow, subluxation of the radial head, and most recently annular ligament displacement, is a common injury in children younger than age 6 years. One study estimates that the condition represented about 1% of injury-related ED visits in 2005.1
Patients with nursemaid’s elbow typically present holding the injured arm at their side, slightly flexed and pronated. These patients appear relatively comfortable until moved actively or passively. The classic history of nursemaid’s elbow includes a traction mechanism, with the child being pulled up by one arm or being grabbed by the arm suddenly to keep him or her out of harm’s way.2 Due to the laxity of connective tissues in children of this age, the head of the radius slips out of the annular ligament causing acute pain and decreased function.
Nursemaid’s elbow is usually diagnosed by history and examination alone, with special consideration to the mechanism of injury. There is rarely swelling or bruising.3 Passive flexion and extension at the elbow may be normal, but rotational maneuvers can be painful or fully resisted.
Reduction Techniques
In 2012, Cochrane updated its earlier review on nursemaid’s elbow and in 2013 followed up with an article in Pediatrics in Review.3,4 Each covered research on reduction techniques, summarizing studies comparing supination-flexion (SF) versus hyperpronation (HP) as the initial reduction maneuver. Given that these maneuvers are difficult to camouflage, studies tend to be pseudorandomized with assessment by a nonblinded healthcare provider, decreasing the strength of the studies. In the Cochrane review, four different trials that included 379 children under age 7 years were selected for the review. In all four studies, pronation was found to have the least chance of failed first attempt, the chosen outcome for this meta-analysis. The risk ratio of failure of reduction for pronation was 0.45 (95% confidence interval [CI], 0.28-0.73).
There is some data supporting hyperpronation to be less painful as well; however, the Cochrane reviewers felt there may have been reporting bias.4 Since the time of each of these reviews, another study comprised of 150 children was conducted and also favored similar practice styles, as the hyperpronation maneuver had 95% success rate on first attempt versus 68% first-time success with supination and flexion.5
Complications and Recurrence
In a small study aimed at identifying recurrence rates for nursemaid’s elbow, Teach and Schultzman6 studied 93 children for 1 year after probable or definite diagnosis of nursemaid’s elbow. Of these children, 23.7% had recurrent radial head subluxation. Children younger than age 2 years were found to have a relative risk of 2.6 (95% CI, 1.04-6.30) for one or more recurrences when compared to children older than age 2 years.
While the great majority of children with nursemaid’s elbow do not need referral to an orthopedist, those with two or more occurrences should be considered for referral to a specialist.
Case 2
A 6-year-old boy was presented to the ED by his father, who had placed the boy’s arm in a home-made sling. The child tearfully told the provider that he fell trying to catch himself after tripping over the house pet.
FOOSH Injury
The above case depicts a very common presentation in the ED—the so-called “FOOSH” (fall onto an outstretched hand) injury. This type of injury occurs with such frequency in both adults and children that it is one of the only injury patterns with a commonly used acronym. The bony injuries seen with FOOSH in children, however, have a different pattern than those in adults.
Pediatric fractures are unique due to the difference in the structure of the bones themselves. A child’s bones are more elastic than an adult’s bones, allowing them to bow and bend before they fracture.7 Despite this malleability, pediatric bones have been noted to have a thicker periosteum. For this reason, compression or impact may interrupt the periosteal sleeve, minimally yielding an incomplete interruption of the cortex unilaterally.
One fracture pattern commonly seen in children is the torus fracture. This type of fracture is also referred to as a buckle fracture as the bone cortex on radiographic imaging appears “buckled” as a result of the compressive forces on that side of the bone (Figure 1). Since the bone itself is minimally affected, these fractures are quite stable and not at risk for complications.
In comparison, a greenstick fracture, also unique to the pediatric population, is one in which the cortex shows plastic deformity on the side of the force or impact but is interrupted on the opposite side due to the tension of the impact itself. Greenstick fractures are frequently angulated and may require reduction for anatomic alignment, but long-term complications are typically minimal. These fracture patterns are distinguished from complete fractures (as seen in adults), which are quite unstable and generally require surgical intervention.
Of note, the location of pediatric forearm fractures varies with age as well. Diaphyseal fractures are more common in prepubescent children, whereas the highest incidence of physeal injuries occurs during large growth spurts, particularly throughout adolescence.7
Management
The remodeling potential of pediatric bones also makes management unique. Pediatric orthopedic literature has well-studied acceptable angles and degrees of appropriate displacement based largely on the age of the patient and proximity to a growth plate. Knowledge of these is imperative for definitive care of such fractures but is beyond the scope of this review.
Traditional treatment of pediatric forearm fractures includes immobilization of various types and duration to minimize pain and deformity while producing the best possible outcome. Several recent studies have aimed to determine best practice for the different fracture types with the goal of producing best alignment and return to function while decreasing cost, discomfort, and number of physician visits. Another concern among healthcare providers is the risk of refracture, which in buckle fractures is estimated at approximately 2% with a median time of 8 to 16 weeks after the initial injury.7
A 2010 review by Kennedy et al8 sought to determine if the refracture rate was affected by the technique used to immobilize torus fractures. The five studies used in this review had no reports of refracture in the 443 patients included in analysis, though only one of the studies (Plint et al) followed patients for more than 6 weeks.8,9 In this study, 75 patients were randomized to either a plaster removable splint or full below-elbow cast for 3 weeks; thereafter, they were followed for 6 months, during which time none experienced refracture.9
Another outcome from the same study assessed the ability of the patient to use the affected arm in the recovery period. While those in removable splints scored better during and immediately after cast removal, no differences were present after 1 week. Not surprisingly, families preferred the soft bandages or a removable splint for treatment.
Case 3
A 13-year-old boy presented to the ED with right ankle pain and difficulty bearing weight. He stated that he was playing basketball when he “rolled” his right ankle coming down from a rebound.
Ankle Fractures
Ankle fractures are among the most common acute injuries of the lower extremity in children, accounting for approximately 5% of pediatric fractures and 15% of physeal injuries.10 Ankle fractures also account for up to 40% of all injuries to the skeletally immature athlete.10,11 More specifically, distal fibular physeal fractures are the most common types of pediatric ankle fracture; however, they are associated with a relatively low risk for long-term complications. In contrast, distal tibial physeal fractures are associated with a higher risk for long-term complications.12,13
Presentation and Evaluation
Typically, patients presenting with ankle fractures are too sore to bear weight, and swelling and ecchymosis can be identified anterior to the ankle. In addition, there may be diffuse tenderness throughout the ankle and point tenderness may be induced on the anterolateral aspect of the distal tibia.14 A complete evaluation of the entire lower extremity should be conducted before assuming that the injury is confined to the ankle, especially in children younger than age 5 years and/or who are nonverbal.10 When evaluating an ankle fracture, in general, orthopedic consultation should be obtained for children with neurovascular compromise, open fractures, and/or Salter-Harris III, IV, and V fractures.
The juvenile Tillaux fracture represents a Salter-Harris III physeal injury that involves the anterolateral portion of the tibia. It usually occurs in children between ages 12 and 14 years as they approach skeletal maturity and who have a partially fused tibial physis. The common mechanism of injury is inversion of the ankle with the foot pointed away from the midline (supination with external rotation). This leads to avulsion of the lateral tibial epiphysis that is attached to the anterior inferior tibiofibular ligament. The uninvolved medial portion of the epiphysis is closed.10
Radiographic Imaging
Three radiographic views should be obtained in the evaluation of pediatric ankle injuries as Tillaux fractures or other subtle injuries could be easily missed if only two views are obtained. Interpretation of the radiographs must be correlated with the physical examination.10 The fracture line is usually best seen on a mortise view (Figure 2). Computed tomography (CT) is warranted in cases in which displacement greater than 2 mm is suspected because it better defines fracture displacement and can aid in surgical planning.14 Because of its sensitivity in detecting fractures displaced more than 2 mm, CT is now the preferred imaging modality in the assessment of juvenile Tillaux fractures.15
Definitive Management
There are two important goals when treating children with ankle fractures—achieving a satisfactory reduction and avoiding physeal arrest so as to minimize the risks of angular deformity, early arthrosis, leg-length inequality, and joint stiffness.11 Juvenile Tillaux fractures with greater than 2 mm of displacement require orthopedic consultation for closed or open reduction. Closed reduction is attempted by internally rotating the foot and applying direct pressure over the anterolateral tibia. If necessary, percutaneous pins can be used for stabilization of the reduction. If closed reduction is unsuccessful, open reduction is required. Care must be taken to assure no displacement occurs after casting; this requires weekly X-ray evaluation for the first 2 weeks.12
Patients with nondisplaced Salter-Harris III fractures are treated with long-leg casting for 4 weeks with conversion to a short-leg cast or boot for an additional 4 weeks. Patients should anticipate 8 weeks of nonweight-bearing. The patient is allowed to remove the boot for range-of-motion exercises but must remain nonweight-bearing for the first 2 weeks.14
Case 4
A 3-year-old previously healthy girl presented to the ED with a limp and difficulty bearing weight. Her mother reported that the child was playing in the yard when she caught her foot on a tree root, stumbled, and fell down. Since the incident, the child has been tearful, limping, and refusing to walk.
Tibial Fractures
Tibial fractures are among the most frequent types of orthopedic injuries in young children, with only femur and forearm fractures having a higher incidence of occurrence. Tibial fractures account for up to 15% of long bone fractures in children and adolescents.16,17 The mechanism of injury varies depending on the patient’s age. In young children, the most common cause of injury is from a seemingly minor twisting around a fixed foot or from a minor fall. In older children and adults, high-energy motor vehicle accidents and sports-related injuries are more common causes.
Fractures of the tibial shaft are typically short oblique or transverse fractures of the middle or distal third of the shaft. Thirty percent of tibial shaft fractures are associated with fractures of the fibula.16
Toddler’s Fracture
The term toddler’s fracture refers to a nondisplaced oblique fracture of the tibial shaft without concomitant fibular fracture. It usually results from an indirect rotational or twisting force applied to the foot and lower leg.16-18 More specifically, the term describes a specialized case of spiral fracture of the distal tibia in patients aged 9 months to 3 years, when weight-bearing is just beginning.19,20 Such injuries commonly occur when a toddler stumbles and falls, or attempts to extricate the foot from between the bars of a crib. Often, however, the mechanism is minimal or unknown.18 Of those injuries that are witnessed, most caregivers report a minor twisting mechanism. Most children with toddler’s fracture are younger than age 6 years. Sixty-three of 76 such fractures reported by Dunbar et al17,19 occurred in children younger than 2.5 years of age. Toddler’s fractures occur more often in boys than girls, and in the right leg more often than the left. Most children will give a history of tripping or twisting their ankle.17
Evaluating the Toddler
Toddlers can be challenging patients as they can not relate history and are often uncooperative on examination. A child may present with a limp, diminished movement of the affected limb, or refuse to bear weight without a distinct history of injury. The onset of limping or refusal to bear weight after minor trauma, or without an obvious injury in a young ambulatory child, warrants a detailed examination looking for tenderness over the tibia, along with radiographic evaluation to rule out a toddler’s fracture.
The examination of the patient is rarely impressive as there is little swelling and bruising with most toddlers’ fractures. A complete clinical history is needed, including a detailed description of any observed traumatic event to exclude the existence of other injuries.
When no traumatic event is observed or an inconsistent history is provided, the physician should obtain a detailed social history, including a list of the child’s most recent caregivers and contacts.16 Because of mild clinical symptoms and frequent lack of a history of injury in this patient population, presentation for evaluation may be delayed. In such cases, by the time the extremity is examined, the fracture has begun to heal. This healing phase may be accompanied by periosteal new bone and, in the absence of a history, may erroneously suggest other, more ominous conditions such as osteomylelitis or tumor.17,18
Consideration of Abuse
Although tibial shaft fractures are rarely found in abused children, diagnosis of child abuse must be considered in cases where a tibial fracture is discovered in the nonambulatory child; his or her clinical history is inconsistent with the injury; and/or there are other physical findings suggestive of abuse. Investigation for suspected nonaccidental trauma includes a thorough physical examination, skeletal survey, and evaluation by social services personnel.16
Radiographic Imaging
Quality anteroposterior (AP) or lateral radiographs of the affected leg may show a hairline fracture, but these can easily be missed on initial plain films in almost a third of patients.21 An internal oblique view can aid in identifying nondisplaced toddler fractures.17 The AP view is the best view for observing the nondisplaced spiral fracture along the distal tibia (Figure 3).6 Occasionally, a fracture line is not identified on initial plain films and the first evidence of fracture becomes apparent on X-ray when new periosteal bone forms 7 to 10 days after the initial injury.
Definitive Treatment
Children with a classic history for a toddler’s fracture and an inability to bear weight should be immobilized with a long-leg splint or cast—even when X-rays are negative—until a definitive diagnosis can be made. Such fractures usually become visible on X-ray 7 to 10 days after injury as a result of new bone growth.22
When definitive diagnosis of a toddler’s fracture is made on plain radiographs, the child should either be immobilized in a long-leg splint with referral to an orthopedist within 5 to 7 days, or immediately casted.16
Conclusion
Fractures in both children and adults are among the most common injury-related presentations to the ED. Based on the structure and increased elasticity of bone in the pediatric patient, there are several fracture patterns unique to this population. Appropriate evaluation, diagnosis, and management in the ED helps to maximize and ensure long-term function and healing while minimizing trauma to the patient.
Dr McBride is an associate professor of pediatrics and pediatric emergency medicine, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
Dr Sutton is a pediatric resident, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
Case 1
A 2-year-old girl presented to the ED with arm pain. Her mother stated that her daughter was playing with a 5-year-old sibling when she heard the child cry- out in pain and noticed she was holding her right arm by her side, not wanting to move it. Neither child gave a reliable story of the injury.
Nursemaid’s Elbow
Nursemaid’s elbow, also known as pulled elbow, subluxation of the radial head, and most recently annular ligament displacement, is a common injury in children younger than age 6 years. One study estimates that the condition represented about 1% of injury-related ED visits in 2005.1
Patients with nursemaid’s elbow typically present holding the injured arm at their side, slightly flexed and pronated. These patients appear relatively comfortable until moved actively or passively. The classic history of nursemaid’s elbow includes a traction mechanism, with the child being pulled up by one arm or being grabbed by the arm suddenly to keep him or her out of harm’s way.2 Due to the laxity of connective tissues in children of this age, the head of the radius slips out of the annular ligament causing acute pain and decreased function.
Nursemaid’s elbow is usually diagnosed by history and examination alone, with special consideration to the mechanism of injury. There is rarely swelling or bruising.3 Passive flexion and extension at the elbow may be normal, but rotational maneuvers can be painful or fully resisted.
Reduction Techniques
In 2012, Cochrane updated its earlier review on nursemaid’s elbow and in 2013 followed up with an article in Pediatrics in Review.3,4 Each covered research on reduction techniques, summarizing studies comparing supination-flexion (SF) versus hyperpronation (HP) as the initial reduction maneuver. Given that these maneuvers are difficult to camouflage, studies tend to be pseudorandomized with assessment by a nonblinded healthcare provider, decreasing the strength of the studies. In the Cochrane review, four different trials that included 379 children under age 7 years were selected for the review. In all four studies, pronation was found to have the least chance of failed first attempt, the chosen outcome for this meta-analysis. The risk ratio of failure of reduction for pronation was 0.45 (95% confidence interval [CI], 0.28-0.73).
There is some data supporting hyperpronation to be less painful as well; however, the Cochrane reviewers felt there may have been reporting bias.4 Since the time of each of these reviews, another study comprised of 150 children was conducted and also favored similar practice styles, as the hyperpronation maneuver had 95% success rate on first attempt versus 68% first-time success with supination and flexion.5
Complications and Recurrence
In a small study aimed at identifying recurrence rates for nursemaid’s elbow, Teach and Schultzman6 studied 93 children for 1 year after probable or definite diagnosis of nursemaid’s elbow. Of these children, 23.7% had recurrent radial head subluxation. Children younger than age 2 years were found to have a relative risk of 2.6 (95% CI, 1.04-6.30) for one or more recurrences when compared to children older than age 2 years.
While the great majority of children with nursemaid’s elbow do not need referral to an orthopedist, those with two or more occurrences should be considered for referral to a specialist.
Case 2
A 6-year-old boy was presented to the ED by his father, who had placed the boy’s arm in a home-made sling. The child tearfully told the provider that he fell trying to catch himself after tripping over the house pet.
FOOSH Injury
The above case depicts a very common presentation in the ED—the so-called “FOOSH” (fall onto an outstretched hand) injury. This type of injury occurs with such frequency in both adults and children that it is one of the only injury patterns with a commonly used acronym. The bony injuries seen with FOOSH in children, however, have a different pattern than those in adults.
Pediatric fractures are unique due to the difference in the structure of the bones themselves. A child’s bones are more elastic than an adult’s bones, allowing them to bow and bend before they fracture.7 Despite this malleability, pediatric bones have been noted to have a thicker periosteum. For this reason, compression or impact may interrupt the periosteal sleeve, minimally yielding an incomplete interruption of the cortex unilaterally.
One fracture pattern commonly seen in children is the torus fracture. This type of fracture is also referred to as a buckle fracture as the bone cortex on radiographic imaging appears “buckled” as a result of the compressive forces on that side of the bone (Figure 1). Since the bone itself is minimally affected, these fractures are quite stable and not at risk for complications.
In comparison, a greenstick fracture, also unique to the pediatric population, is one in which the cortex shows plastic deformity on the side of the force or impact but is interrupted on the opposite side due to the tension of the impact itself. Greenstick fractures are frequently angulated and may require reduction for anatomic alignment, but long-term complications are typically minimal. These fracture patterns are distinguished from complete fractures (as seen in adults), which are quite unstable and generally require surgical intervention.
Of note, the location of pediatric forearm fractures varies with age as well. Diaphyseal fractures are more common in prepubescent children, whereas the highest incidence of physeal injuries occurs during large growth spurts, particularly throughout adolescence.7
Management
The remodeling potential of pediatric bones also makes management unique. Pediatric orthopedic literature has well-studied acceptable angles and degrees of appropriate displacement based largely on the age of the patient and proximity to a growth plate. Knowledge of these is imperative for definitive care of such fractures but is beyond the scope of this review.
Traditional treatment of pediatric forearm fractures includes immobilization of various types and duration to minimize pain and deformity while producing the best possible outcome. Several recent studies have aimed to determine best practice for the different fracture types with the goal of producing best alignment and return to function while decreasing cost, discomfort, and number of physician visits. Another concern among healthcare providers is the risk of refracture, which in buckle fractures is estimated at approximately 2% with a median time of 8 to 16 weeks after the initial injury.7
A 2010 review by Kennedy et al8 sought to determine if the refracture rate was affected by the technique used to immobilize torus fractures. The five studies used in this review had no reports of refracture in the 443 patients included in analysis, though only one of the studies (Plint et al) followed patients for more than 6 weeks.8,9 In this study, 75 patients were randomized to either a plaster removable splint or full below-elbow cast for 3 weeks; thereafter, they were followed for 6 months, during which time none experienced refracture.9
Another outcome from the same study assessed the ability of the patient to use the affected arm in the recovery period. While those in removable splints scored better during and immediately after cast removal, no differences were present after 1 week. Not surprisingly, families preferred the soft bandages or a removable splint for treatment.
Case 3
A 13-year-old boy presented to the ED with right ankle pain and difficulty bearing weight. He stated that he was playing basketball when he “rolled” his right ankle coming down from a rebound.
Ankle Fractures
Ankle fractures are among the most common acute injuries of the lower extremity in children, accounting for approximately 5% of pediatric fractures and 15% of physeal injuries.10 Ankle fractures also account for up to 40% of all injuries to the skeletally immature athlete.10,11 More specifically, distal fibular physeal fractures are the most common types of pediatric ankle fracture; however, they are associated with a relatively low risk for long-term complications. In contrast, distal tibial physeal fractures are associated with a higher risk for long-term complications.12,13
Presentation and Evaluation
Typically, patients presenting with ankle fractures are too sore to bear weight, and swelling and ecchymosis can be identified anterior to the ankle. In addition, there may be diffuse tenderness throughout the ankle and point tenderness may be induced on the anterolateral aspect of the distal tibia.14 A complete evaluation of the entire lower extremity should be conducted before assuming that the injury is confined to the ankle, especially in children younger than age 5 years and/or who are nonverbal.10 When evaluating an ankle fracture, in general, orthopedic consultation should be obtained for children with neurovascular compromise, open fractures, and/or Salter-Harris III, IV, and V fractures.
The juvenile Tillaux fracture represents a Salter-Harris III physeal injury that involves the anterolateral portion of the tibia. It usually occurs in children between ages 12 and 14 years as they approach skeletal maturity and who have a partially fused tibial physis. The common mechanism of injury is inversion of the ankle with the foot pointed away from the midline (supination with external rotation). This leads to avulsion of the lateral tibial epiphysis that is attached to the anterior inferior tibiofibular ligament. The uninvolved medial portion of the epiphysis is closed.10
Radiographic Imaging
Three radiographic views should be obtained in the evaluation of pediatric ankle injuries as Tillaux fractures or other subtle injuries could be easily missed if only two views are obtained. Interpretation of the radiographs must be correlated with the physical examination.10 The fracture line is usually best seen on a mortise view (Figure 2). Computed tomography (CT) is warranted in cases in which displacement greater than 2 mm is suspected because it better defines fracture displacement and can aid in surgical planning.14 Because of its sensitivity in detecting fractures displaced more than 2 mm, CT is now the preferred imaging modality in the assessment of juvenile Tillaux fractures.15
Definitive Management
There are two important goals when treating children with ankle fractures—achieving a satisfactory reduction and avoiding physeal arrest so as to minimize the risks of angular deformity, early arthrosis, leg-length inequality, and joint stiffness.11 Juvenile Tillaux fractures with greater than 2 mm of displacement require orthopedic consultation for closed or open reduction. Closed reduction is attempted by internally rotating the foot and applying direct pressure over the anterolateral tibia. If necessary, percutaneous pins can be used for stabilization of the reduction. If closed reduction is unsuccessful, open reduction is required. Care must be taken to assure no displacement occurs after casting; this requires weekly X-ray evaluation for the first 2 weeks.12
Patients with nondisplaced Salter-Harris III fractures are treated with long-leg casting for 4 weeks with conversion to a short-leg cast or boot for an additional 4 weeks. Patients should anticipate 8 weeks of nonweight-bearing. The patient is allowed to remove the boot for range-of-motion exercises but must remain nonweight-bearing for the first 2 weeks.14
Case 4
A 3-year-old previously healthy girl presented to the ED with a limp and difficulty bearing weight. Her mother reported that the child was playing in the yard when she caught her foot on a tree root, stumbled, and fell down. Since the incident, the child has been tearful, limping, and refusing to walk.
Tibial Fractures
Tibial fractures are among the most frequent types of orthopedic injuries in young children, with only femur and forearm fractures having a higher incidence of occurrence. Tibial fractures account for up to 15% of long bone fractures in children and adolescents.16,17 The mechanism of injury varies depending on the patient’s age. In young children, the most common cause of injury is from a seemingly minor twisting around a fixed foot or from a minor fall. In older children and adults, high-energy motor vehicle accidents and sports-related injuries are more common causes.
Fractures of the tibial shaft are typically short oblique or transverse fractures of the middle or distal third of the shaft. Thirty percent of tibial shaft fractures are associated with fractures of the fibula.16
Toddler’s Fracture
The term toddler’s fracture refers to a nondisplaced oblique fracture of the tibial shaft without concomitant fibular fracture. It usually results from an indirect rotational or twisting force applied to the foot and lower leg.16-18 More specifically, the term describes a specialized case of spiral fracture of the distal tibia in patients aged 9 months to 3 years, when weight-bearing is just beginning.19,20 Such injuries commonly occur when a toddler stumbles and falls, or attempts to extricate the foot from between the bars of a crib. Often, however, the mechanism is minimal or unknown.18 Of those injuries that are witnessed, most caregivers report a minor twisting mechanism. Most children with toddler’s fracture are younger than age 6 years. Sixty-three of 76 such fractures reported by Dunbar et al17,19 occurred in children younger than 2.5 years of age. Toddler’s fractures occur more often in boys than girls, and in the right leg more often than the left. Most children will give a history of tripping or twisting their ankle.17
Evaluating the Toddler
Toddlers can be challenging patients as they can not relate history and are often uncooperative on examination. A child may present with a limp, diminished movement of the affected limb, or refuse to bear weight without a distinct history of injury. The onset of limping or refusal to bear weight after minor trauma, or without an obvious injury in a young ambulatory child, warrants a detailed examination looking for tenderness over the tibia, along with radiographic evaluation to rule out a toddler’s fracture.
The examination of the patient is rarely impressive as there is little swelling and bruising with most toddlers’ fractures. A complete clinical history is needed, including a detailed description of any observed traumatic event to exclude the existence of other injuries.
When no traumatic event is observed or an inconsistent history is provided, the physician should obtain a detailed social history, including a list of the child’s most recent caregivers and contacts.16 Because of mild clinical symptoms and frequent lack of a history of injury in this patient population, presentation for evaluation may be delayed. In such cases, by the time the extremity is examined, the fracture has begun to heal. This healing phase may be accompanied by periosteal new bone and, in the absence of a history, may erroneously suggest other, more ominous conditions such as osteomylelitis or tumor.17,18
Consideration of Abuse
Although tibial shaft fractures are rarely found in abused children, diagnosis of child abuse must be considered in cases where a tibial fracture is discovered in the nonambulatory child; his or her clinical history is inconsistent with the injury; and/or there are other physical findings suggestive of abuse. Investigation for suspected nonaccidental trauma includes a thorough physical examination, skeletal survey, and evaluation by social services personnel.16
Radiographic Imaging
Quality anteroposterior (AP) or lateral radiographs of the affected leg may show a hairline fracture, but these can easily be missed on initial plain films in almost a third of patients.21 An internal oblique view can aid in identifying nondisplaced toddler fractures.17 The AP view is the best view for observing the nondisplaced spiral fracture along the distal tibia (Figure 3).6 Occasionally, a fracture line is not identified on initial plain films and the first evidence of fracture becomes apparent on X-ray when new periosteal bone forms 7 to 10 days after the initial injury.
Definitive Treatment
Children with a classic history for a toddler’s fracture and an inability to bear weight should be immobilized with a long-leg splint or cast—even when X-rays are negative—until a definitive diagnosis can be made. Such fractures usually become visible on X-ray 7 to 10 days after injury as a result of new bone growth.22
When definitive diagnosis of a toddler’s fracture is made on plain radiographs, the child should either be immobilized in a long-leg splint with referral to an orthopedist within 5 to 7 days, or immediately casted.16
Conclusion
Fractures in both children and adults are among the most common injury-related presentations to the ED. Based on the structure and increased elasticity of bone in the pediatric patient, there are several fracture patterns unique to this population. Appropriate evaluation, diagnosis, and management in the ED helps to maximize and ensure long-term function and healing while minimizing trauma to the patient.
Dr McBride is an associate professor of pediatrics and pediatric emergency medicine, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
Dr Sutton is a pediatric resident, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
- Brown D. Emergency department visits for nursemaid’s elbow in the United States, 2005-2006. Orthop Nurs. 2009;28(4):161,162.
- Hardy RH. Pulled elbow. J R Coll Gen Pract. 1978;28(189):224-226.
- Browner EA. Nursemaid’s elbow (annular ligament displacement). Pediatr Rev. 2013;34(8):366,367.
- Krul M, van der Wouden JC,van Suijlekom-Smit LW, Koes BM. Manipulative interventions for reducing pulled elbow in young children. Cochrane Database of Syst Rev. 2012;1:CD007759.
- Gunaydin YK, Katirci Y, Duymaz H, et al. Comparison of success and pain levels of supination-flexion and hyperpronation maneuvers in childhood nursemaid’s elbow cases. Am J Emerg Med. 2013;31(7):1078-1081.
- Teach SJ, Schutzman SA. Prospective study of recurrent radial head subluxation. Arch Pediatr Adolesc Med. 1996;150(2):164-166.
- Dolan M and Waters PM. Fractures and dislocations of the forearm, wrist, and hand. In: Green NE, Swiontkowski MF, eds. Skeletal Trauma in Children. 4th ed. Philadephia, PA: Saunders Elsevier; 2009:159-206.
- Kennedy SA, Slobogean GP, Mulpuri K. Does degree of immobilization influence refracture rate in the forearm buckle fracture? J Pediatr Orthop B. 2010;19(1):77-81.
- Plint AC, Perry JJ, Correll R, Gaboury I, Lawtown L. A randomized, controlled trial of removable splinting versus casting for wrist buckle fractures in children. Pediatrics. 2006;117(3):691-697.
- Kay RM, Matthys GA. Pediatric ankle fractures: evaluation and treatment. J Am Acad Orthop Surg. 2001;9(4):268-278.
- Marsh JS, Daigneault JP. Ankle injuries in the pediatric population. Curr Opin Pediatr. 2000;12(1):52-60
- Cummings RJ. Distal tibial and fibular fractures. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins’ Fractures in Children. 6th ed. Pennsylvania, PA: Lippincott Williams & Wilkins; 2006:1096-1104.
- Boutis K, Willan AR, Babyn P, Narayanan UG, Alman B, Schuh S. A randomized, controlled trial of a removable brace versus casting in children with low-risk ankle fractures. Pediatrics. 2007;119(6):1256-1263.
- Wuerz TH, Gurd DP. Pediatric physeal ankle fracture. J Am Acad Orthop Surg. 2013;21(4):234-244.
- Horn BD, Crisci K, Krug M, Pizzutillo PD, MacEwen GD. Radiologic evaluation of juvenile Tillaux fractures of the distal tibia. J Pediatr Orthop. 2001;21(2):162-164.
- Mashru RP, Herman MJ, Pizzutillo PD. Tibial shaft fractures in children and adolescents. J Am Acad Orthop Surg. 2005;139(5):345-352.
- Heinrich SD, Mooney JF. Fractures of the shaft of the tibia and fibula. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins’ Fractures in Children. 6th ed. Pennsylvania, PA: Lippincott Williams & Wilkins; 2006:1063,1064.
- John SD, Moorthy CS, Swischuk LE. Expanding the concept of the toddler’s fracture. Radiographics. 1997;17(2):367-376.
- Dunbar JS, Owen HF, Nogrady MB, McLeese R. Obscure tibial fracture of infants—the toddlers’ fracture. J Can Assoc Radiol 1964;15:136-144.
- Tenenbein M, Reed MH, Black GB. The toddler’s fracture revisited. Am J Emerg Med. 1990;8(3):208-211.
- Shravat BP, Harrop SN, Kane TP. Toddler’s fracture. J Accid Emerg Med. 1996;13(1):59-61.
- Halsey MF, Finzel KC, Carrion WV, Haralabatos SS, Gruber MA, Meinhard BP. Toddler’s fracture: presumptive diagnosis and treatment. J Pediatr Orthop. 2001;21(2):152-156.
- Brown D. Emergency department visits for nursemaid’s elbow in the United States, 2005-2006. Orthop Nurs. 2009;28(4):161,162.
- Hardy RH. Pulled elbow. J R Coll Gen Pract. 1978;28(189):224-226.
- Browner EA. Nursemaid’s elbow (annular ligament displacement). Pediatr Rev. 2013;34(8):366,367.
- Krul M, van der Wouden JC,van Suijlekom-Smit LW, Koes BM. Manipulative interventions for reducing pulled elbow in young children. Cochrane Database of Syst Rev. 2012;1:CD007759.
- Gunaydin YK, Katirci Y, Duymaz H, et al. Comparison of success and pain levels of supination-flexion and hyperpronation maneuvers in childhood nursemaid’s elbow cases. Am J Emerg Med. 2013;31(7):1078-1081.
- Teach SJ, Schutzman SA. Prospective study of recurrent radial head subluxation. Arch Pediatr Adolesc Med. 1996;150(2):164-166.
- Dolan M and Waters PM. Fractures and dislocations of the forearm, wrist, and hand. In: Green NE, Swiontkowski MF, eds. Skeletal Trauma in Children. 4th ed. Philadephia, PA: Saunders Elsevier; 2009:159-206.
- Kennedy SA, Slobogean GP, Mulpuri K. Does degree of immobilization influence refracture rate in the forearm buckle fracture? J Pediatr Orthop B. 2010;19(1):77-81.
- Plint AC, Perry JJ, Correll R, Gaboury I, Lawtown L. A randomized, controlled trial of removable splinting versus casting for wrist buckle fractures in children. Pediatrics. 2006;117(3):691-697.
- Kay RM, Matthys GA. Pediatric ankle fractures: evaluation and treatment. J Am Acad Orthop Surg. 2001;9(4):268-278.
- Marsh JS, Daigneault JP. Ankle injuries in the pediatric population. Curr Opin Pediatr. 2000;12(1):52-60
- Cummings RJ. Distal tibial and fibular fractures. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins’ Fractures in Children. 6th ed. Pennsylvania, PA: Lippincott Williams & Wilkins; 2006:1096-1104.
- Boutis K, Willan AR, Babyn P, Narayanan UG, Alman B, Schuh S. A randomized, controlled trial of a removable brace versus casting in children with low-risk ankle fractures. Pediatrics. 2007;119(6):1256-1263.
- Wuerz TH, Gurd DP. Pediatric physeal ankle fracture. J Am Acad Orthop Surg. 2013;21(4):234-244.
- Horn BD, Crisci K, Krug M, Pizzutillo PD, MacEwen GD. Radiologic evaluation of juvenile Tillaux fractures of the distal tibia. J Pediatr Orthop. 2001;21(2):162-164.
- Mashru RP, Herman MJ, Pizzutillo PD. Tibial shaft fractures in children and adolescents. J Am Acad Orthop Surg. 2005;139(5):345-352.
- Heinrich SD, Mooney JF. Fractures of the shaft of the tibia and fibula. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkins’ Fractures in Children. 6th ed. Pennsylvania, PA: Lippincott Williams & Wilkins; 2006:1063,1064.
- John SD, Moorthy CS, Swischuk LE. Expanding the concept of the toddler’s fracture. Radiographics. 1997;17(2):367-376.
- Dunbar JS, Owen HF, Nogrady MB, McLeese R. Obscure tibial fracture of infants—the toddlers’ fracture. J Can Assoc Radiol 1964;15:136-144.
- Tenenbein M, Reed MH, Black GB. The toddler’s fracture revisited. Am J Emerg Med. 1990;8(3):208-211.
- Shravat BP, Harrop SN, Kane TP. Toddler’s fracture. J Accid Emerg Med. 1996;13(1):59-61.
- Halsey MF, Finzel KC, Carrion WV, Haralabatos SS, Gruber MA, Meinhard BP. Toddler’s fracture: presumptive diagnosis and treatment. J Pediatr Orthop. 2001;21(2):152-156.
