User login
Clinical Psychiatry News is the online destination and multimedia properties of Clinica Psychiatry News, the independent news publication for psychiatrists. Since 1971, Clinical Psychiatry News has been the leading source of news and commentary about clinical developments in psychiatry as well as health care policy and regulations that affect the physician's practice.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
ketamine
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
suicide
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-cpn')]
div[contains(@class, 'pane-pub-home-cpn')]
div[contains(@class, 'pane-pub-topic-cpn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Getting Patients With Opioid Use Disorder Started on Buprenorphine in Primary Care
*The first thing Ann Garment, MD, wants all clinicians to know about buprenorphine is that [where state law permits] any prescriber with a DEA registration number “is able to prescribe buprenorphine and should be ready and willing to prescribe” the medication.
*A change in federal law means that for most providers “there is no longer any extra paperwork or training required to prescribe buprenorphine,” said Dr. Garment, clinical associate professor at New York University and chief of general internal medicine at Bellevue Hospital in New York City, during a presentation on April 19 at the American College of Physicians (ACP-IM) Internal Medicine Meeting 2024.
Dr. Garment, who specializes in opioid use disorder (OUD), described the current “third wave” of increasing opioid overdose deaths fueled by the increase of synthetic opioids in the drug supply. The third wave started in 2013 with the rise in use of fentanyl and tramadol. The 107,000 number of overdose deaths in the United States in 2021 was more than six times that in 1999, and 75% involved opioids.
“Now, more than ever,” Dr. Garment said, “opioid use disorder should be treated from the primary care setting.”
How to Identify OUD
“It’s less sensitive for picking up on people who have a prior opioid use disorder history or are only exhibiting risky opioid use that wouldn’t constitute opioid use disorder yet,” she said.
If someone screens positive, to verify OUD, the Diagnostic and Statistical Manual of Mental Disorders identifies criteria for any substance abuse disorder with two general themes: Loss of control and continued use despite negative consequences.
“If you have a patient who is getting prescribed opioids and they have opioid tolerance or withdrawal, that does not mean they have opioid use disorder,” she said.
Medication for OUD
Medication is the top treatment for OUD, according to Dr. Garment. Psychosocial treatments can help some but not all people with OUD, she said. “It is not a requirement for a patient to engage in psychosocial treatment in order to get a medication for opioid use disorder, so please do not let that be a barrier for your patients,” she said.
Buprenorphine has advantages over other medications for OUD, including methadone and naltrexone.
Methadone must be obtained daily at a methadone clinic instead of at a local pharmacy. And escalating doses of methadone carry an increased risk for overdose and respiratory problems and potential drug-drug interactions, Dr. Garment added.
One downside with naltrexone is loss of tolerance, she said. If a patient has been using naltrexone to treat OUD and they decide to resume taking opioids, “they no longer can use the same amount of opioids that they were using before” because they have lost their tolerance and now are at a risk for overdose with their usual amount, she said. What’s more, naltrexone has not been shown to reduce overdose deaths.
Finally, she said, buprenorphine, “is an incredibly safe medication. If anyone in this room has ever prescribed coumadin or insulin, I’m going to tell you: This is much safer.”
Dr. Garment offered three reasons for buprenorphine’s safety:
- The drug is a partial, as opposed to full, opioid agonist, so as the dose increases, the patient experiences less withdrawal and fewer opioid cravings. As a result, they will hit a ceiling effect that avoids euphoria, respiratory depression, or overdose.
- Buprenorphine is “stickier” than other OUD medications: “If I’m taking buprenorphine and I decide to use some [oxycodone], what’s going to happen is that very little of that, if any, is going to get bound to my opioid receptors because buprenorphine is so sticky and adherent, it’s not going to let other opioids on.”
- Most buprenorphine is co-formulated with naloxone, an opioid antagonist. If a patient tries to get high from buprenorphine and tries to snort or inject it, naloxone will kick in and cancel out the buprenorphine.
Dr. Garment said she obtains urine screens ideally twice a year. If other drugs show up on the test, she said, she speaks with the patient about their drug use. “It’s never a reason to discharge someone from a practice,” she said.
Dr. Garment reported no relevant financial conflicts of interest.
*This story was updated on April 29, 2024.
A version of this article appeared on Medscape.com.
*The first thing Ann Garment, MD, wants all clinicians to know about buprenorphine is that [where state law permits] any prescriber with a DEA registration number “is able to prescribe buprenorphine and should be ready and willing to prescribe” the medication.
*A change in federal law means that for most providers “there is no longer any extra paperwork or training required to prescribe buprenorphine,” said Dr. Garment, clinical associate professor at New York University and chief of general internal medicine at Bellevue Hospital in New York City, during a presentation on April 19 at the American College of Physicians (ACP-IM) Internal Medicine Meeting 2024.
Dr. Garment, who specializes in opioid use disorder (OUD), described the current “third wave” of increasing opioid overdose deaths fueled by the increase of synthetic opioids in the drug supply. The third wave started in 2013 with the rise in use of fentanyl and tramadol. The 107,000 number of overdose deaths in the United States in 2021 was more than six times that in 1999, and 75% involved opioids.
“Now, more than ever,” Dr. Garment said, “opioid use disorder should be treated from the primary care setting.”
How to Identify OUD
“It’s less sensitive for picking up on people who have a prior opioid use disorder history or are only exhibiting risky opioid use that wouldn’t constitute opioid use disorder yet,” she said.
If someone screens positive, to verify OUD, the Diagnostic and Statistical Manual of Mental Disorders identifies criteria for any substance abuse disorder with two general themes: Loss of control and continued use despite negative consequences.
“If you have a patient who is getting prescribed opioids and they have opioid tolerance or withdrawal, that does not mean they have opioid use disorder,” she said.
Medication for OUD
Medication is the top treatment for OUD, according to Dr. Garment. Psychosocial treatments can help some but not all people with OUD, she said. “It is not a requirement for a patient to engage in psychosocial treatment in order to get a medication for opioid use disorder, so please do not let that be a barrier for your patients,” she said.
Buprenorphine has advantages over other medications for OUD, including methadone and naltrexone.
Methadone must be obtained daily at a methadone clinic instead of at a local pharmacy. And escalating doses of methadone carry an increased risk for overdose and respiratory problems and potential drug-drug interactions, Dr. Garment added.
One downside with naltrexone is loss of tolerance, she said. If a patient has been using naltrexone to treat OUD and they decide to resume taking opioids, “they no longer can use the same amount of opioids that they were using before” because they have lost their tolerance and now are at a risk for overdose with their usual amount, she said. What’s more, naltrexone has not been shown to reduce overdose deaths.
Finally, she said, buprenorphine, “is an incredibly safe medication. If anyone in this room has ever prescribed coumadin or insulin, I’m going to tell you: This is much safer.”
Dr. Garment offered three reasons for buprenorphine’s safety:
- The drug is a partial, as opposed to full, opioid agonist, so as the dose increases, the patient experiences less withdrawal and fewer opioid cravings. As a result, they will hit a ceiling effect that avoids euphoria, respiratory depression, or overdose.
- Buprenorphine is “stickier” than other OUD medications: “If I’m taking buprenorphine and I decide to use some [oxycodone], what’s going to happen is that very little of that, if any, is going to get bound to my opioid receptors because buprenorphine is so sticky and adherent, it’s not going to let other opioids on.”
- Most buprenorphine is co-formulated with naloxone, an opioid antagonist. If a patient tries to get high from buprenorphine and tries to snort or inject it, naloxone will kick in and cancel out the buprenorphine.
Dr. Garment said she obtains urine screens ideally twice a year. If other drugs show up on the test, she said, she speaks with the patient about their drug use. “It’s never a reason to discharge someone from a practice,” she said.
Dr. Garment reported no relevant financial conflicts of interest.
*This story was updated on April 29, 2024.
A version of this article appeared on Medscape.com.
*The first thing Ann Garment, MD, wants all clinicians to know about buprenorphine is that [where state law permits] any prescriber with a DEA registration number “is able to prescribe buprenorphine and should be ready and willing to prescribe” the medication.
*A change in federal law means that for most providers “there is no longer any extra paperwork or training required to prescribe buprenorphine,” said Dr. Garment, clinical associate professor at New York University and chief of general internal medicine at Bellevue Hospital in New York City, during a presentation on April 19 at the American College of Physicians (ACP-IM) Internal Medicine Meeting 2024.
Dr. Garment, who specializes in opioid use disorder (OUD), described the current “third wave” of increasing opioid overdose deaths fueled by the increase of synthetic opioids in the drug supply. The third wave started in 2013 with the rise in use of fentanyl and tramadol. The 107,000 number of overdose deaths in the United States in 2021 was more than six times that in 1999, and 75% involved opioids.
“Now, more than ever,” Dr. Garment said, “opioid use disorder should be treated from the primary care setting.”
How to Identify OUD
“It’s less sensitive for picking up on people who have a prior opioid use disorder history or are only exhibiting risky opioid use that wouldn’t constitute opioid use disorder yet,” she said.
If someone screens positive, to verify OUD, the Diagnostic and Statistical Manual of Mental Disorders identifies criteria for any substance abuse disorder with two general themes: Loss of control and continued use despite negative consequences.
“If you have a patient who is getting prescribed opioids and they have opioid tolerance or withdrawal, that does not mean they have opioid use disorder,” she said.
Medication for OUD
Medication is the top treatment for OUD, according to Dr. Garment. Psychosocial treatments can help some but not all people with OUD, she said. “It is not a requirement for a patient to engage in psychosocial treatment in order to get a medication for opioid use disorder, so please do not let that be a barrier for your patients,” she said.
Buprenorphine has advantages over other medications for OUD, including methadone and naltrexone.
Methadone must be obtained daily at a methadone clinic instead of at a local pharmacy. And escalating doses of methadone carry an increased risk for overdose and respiratory problems and potential drug-drug interactions, Dr. Garment added.
One downside with naltrexone is loss of tolerance, she said. If a patient has been using naltrexone to treat OUD and they decide to resume taking opioids, “they no longer can use the same amount of opioids that they were using before” because they have lost their tolerance and now are at a risk for overdose with their usual amount, she said. What’s more, naltrexone has not been shown to reduce overdose deaths.
Finally, she said, buprenorphine, “is an incredibly safe medication. If anyone in this room has ever prescribed coumadin or insulin, I’m going to tell you: This is much safer.”
Dr. Garment offered three reasons for buprenorphine’s safety:
- The drug is a partial, as opposed to full, opioid agonist, so as the dose increases, the patient experiences less withdrawal and fewer opioid cravings. As a result, they will hit a ceiling effect that avoids euphoria, respiratory depression, or overdose.
- Buprenorphine is “stickier” than other OUD medications: “If I’m taking buprenorphine and I decide to use some [oxycodone], what’s going to happen is that very little of that, if any, is going to get bound to my opioid receptors because buprenorphine is so sticky and adherent, it’s not going to let other opioids on.”
- Most buprenorphine is co-formulated with naloxone, an opioid antagonist. If a patient tries to get high from buprenorphine and tries to snort or inject it, naloxone will kick in and cancel out the buprenorphine.
Dr. Garment said she obtains urine screens ideally twice a year. If other drugs show up on the test, she said, she speaks with the patient about their drug use. “It’s never a reason to discharge someone from a practice,” she said.
Dr. Garment reported no relevant financial conflicts of interest.
*This story was updated on April 29, 2024.
A version of this article appeared on Medscape.com.
Are Women Better Doctors Than Men?
This transcript has been edited for clarity.
It’s a battle of the sexes today as we dive into a paper that makes you say, “Wow, what an interesting study” and also “Boy, am I glad I didn’t do that study.” That’s because studies like this are always somewhat fraught; they say something about medicine but also something about society — and that makes this a bit precarious. But that’s never stopped us before. So, let’s go ahead and try to answer the question: Do women make better doctors than men?
On the surface, this question seems nearly impossible to answer. It’s too broad; what does it mean to be a “better” doctor? At first blush it seems that there are just too many variables to control for here: the type of doctor, the type of patient, the clinical scenario, and so on.
But this study, “Comparison of hospital mortality and readmission rates by physician and patient sex,” which appears in Annals of Internal Medicine, uses a fairly ingenious method to cut through all the bias by leveraging two simple facts: First, hospital medicine is largely conducted by hospitalists these days; second, due to the shift-based nature of hospitalist work, the hospitalist you get when you are admitted to the hospital is pretty much random.
In other words, if you are admitted to the hospital for an acute illness and get a hospitalist as your attending, you have no control over whether it is a man or a woman. Is this a randomized trial? No, but it’s not bad.
Researchers used Medicare claims data to identify adults over age 65 who had nonelective hospital admissions throughout the United States. The claims revealed the sex of the patient and the name of the attending physician. By linking to a medical provider database, they could determine the sex of the provider.
The goal was to look at outcomes across four dyads:
- Male patient – male doctor
- Male patient – female doctor
- Female patient – male doctor
- Female patient – female doctor
The primary outcome was 30-day mortality.
I told you that focusing on hospitalists produces some pseudorandomization, but let’s look at the data to be sure. Just under a million patients were treated by approximately 50,000 physicians, 30% of whom were female. And, though female patients and male patients differed, they did not differ with respect to the sex of their hospitalist. So, by physician sex, patients were similar in mean age, race, ethnicity, household income, eligibility for Medicaid, and comorbid conditions. The authors even created a “predicted mortality” score which was similar across the groups as well.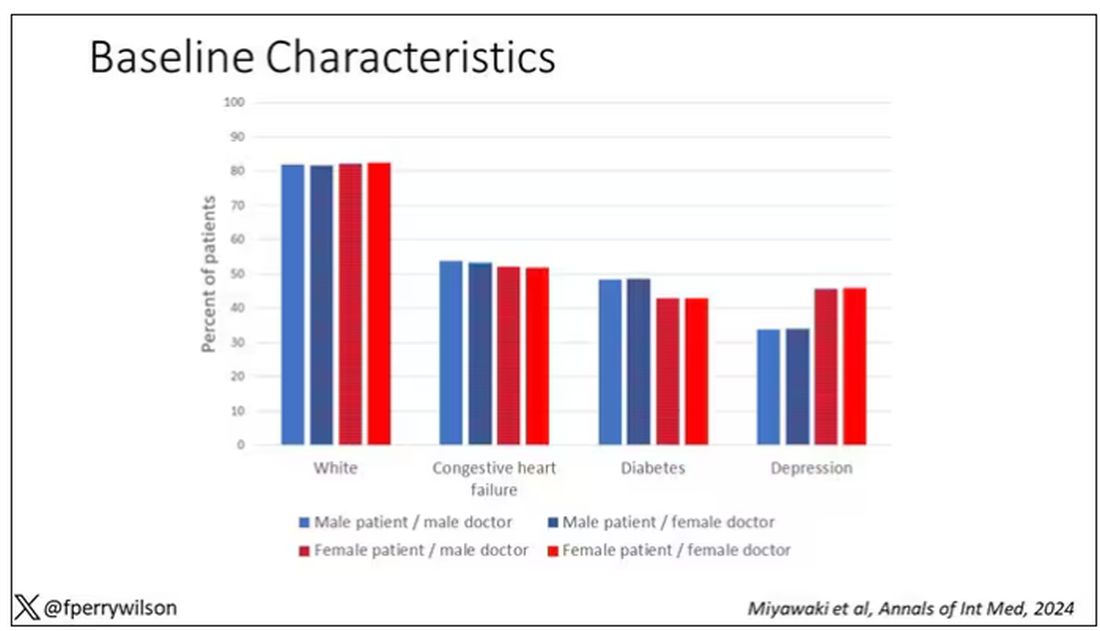
Now, the female physicians were a bit different from the male physicians. The female hospitalists were slightly more likely to have an osteopathic degree, had slightly fewer admissions per year, and were a bit younger.
So, we have broadly similar patients regardless of who their hospitalist was, but hospitalists differ by factors other than their sex. Fine.
I’ve graphed the results here. 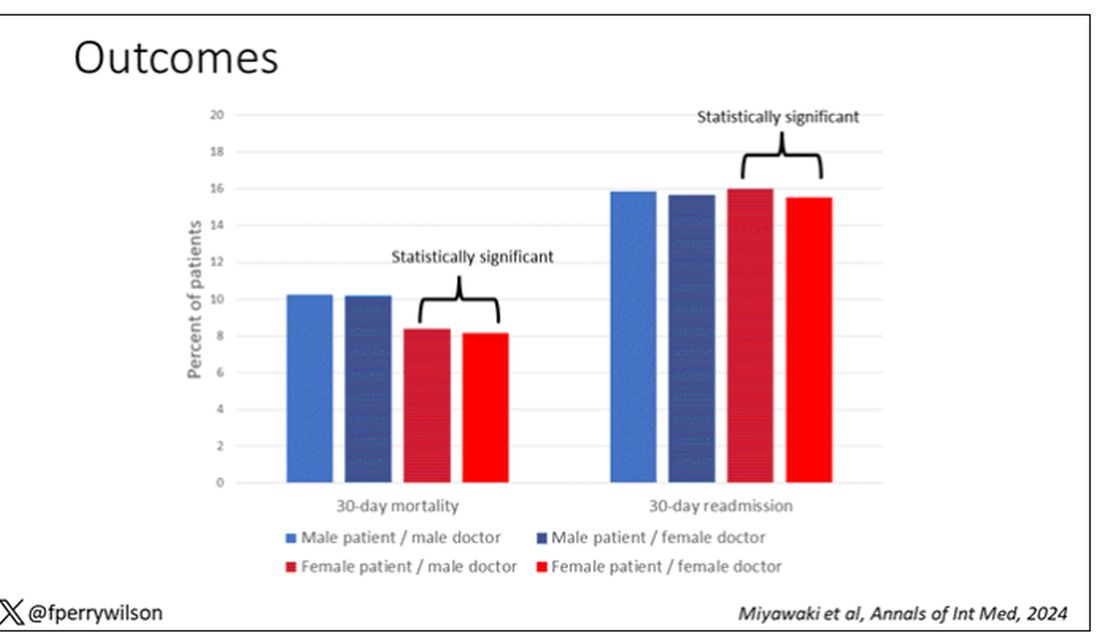
This is a relatively small effect, to be sure, but if you multiply it across the millions of hospitalist admissions per year, you can start to put up some real numbers.
So, what is going on here? I see four broad buckets of possibilities.
Let’s start with the obvious explanation: Women, on average, are better doctors than men. I am married to a woman doctor, and based on my personal experience, this explanation is undoubtedly true. But why would that be?
The authors cite data that suggest that female physicians are less likely than male physicians to dismiss patient concerns — and in particular, the concerns of female patients — perhaps leading to fewer missed diagnoses. But this is impossible to measure with administrative data, so this study can no more tell us whether these female hospitalists are more attentive than their male counterparts than it can suggest that the benefit is mediated by the shorter average height of female physicians. Perhaps the key is being closer to the patient?
The second possibility here is that this has nothing to do with the sex of the physician at all; it has to do with those other things that associate with the sex of the physician. We know, for example, that the female physicians saw fewer patients per year than the male physicians, but the study authors adjusted for this in the statistical models. Still, other unmeasured factors (confounders) could be present. By the way, confounders wouldn’t necessarily change the primary finding — you are better off being cared for by female physicians. It’s just not because they are female; it’s a convenient marker for some other quality, such as age.
The third possibility is that the study represents a phenomenon called collider bias. The idea here is that physicians only get into the study if they are hospitalists, and the quality of physicians who choose to become a hospitalist may differ by sex. When deciding on a specialty, a talented resident considering certain lifestyle issues may find hospital medicine particularly attractive — and that draw toward a more lifestyle-friendly specialty may differ by sex, as some prior studies have shown. If true, the pool of women hospitalists may be better than their male counterparts because male physicians of that caliber don’t become hospitalists.
Okay, don’t write in. I’m just trying to cite examples of how to think about collider bias. I can’t prove that this is the case, and in fact the authors do a sensitivity analysis of all physicians, not just hospitalists, and show the same thing. So this is probably not true, but epidemiology is fun, right?
And the fourth possibility: This is nothing but statistical noise. The effect size is incredibly small and just on the border of statistical significance. Especially when you’re working with very large datasets like this, you’ve got to be really careful about overinterpreting statistically significant findings that are nevertheless of small magnitude.
Regardless, it’s an interesting study, one that made me think and, of course, worry a bit about how I would present it. Forgive me if I’ve been indelicate in handling the complex issues of sex, gender, and society here. But I’m not sure what you expect; after all, I’m only a male doctor.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It’s a battle of the sexes today as we dive into a paper that makes you say, “Wow, what an interesting study” and also “Boy, am I glad I didn’t do that study.” That’s because studies like this are always somewhat fraught; they say something about medicine but also something about society — and that makes this a bit precarious. But that’s never stopped us before. So, let’s go ahead and try to answer the question: Do women make better doctors than men?
On the surface, this question seems nearly impossible to answer. It’s too broad; what does it mean to be a “better” doctor? At first blush it seems that there are just too many variables to control for here: the type of doctor, the type of patient, the clinical scenario, and so on.
But this study, “Comparison of hospital mortality and readmission rates by physician and patient sex,” which appears in Annals of Internal Medicine, uses a fairly ingenious method to cut through all the bias by leveraging two simple facts: First, hospital medicine is largely conducted by hospitalists these days; second, due to the shift-based nature of hospitalist work, the hospitalist you get when you are admitted to the hospital is pretty much random.
In other words, if you are admitted to the hospital for an acute illness and get a hospitalist as your attending, you have no control over whether it is a man or a woman. Is this a randomized trial? No, but it’s not bad.
Researchers used Medicare claims data to identify adults over age 65 who had nonelective hospital admissions throughout the United States. The claims revealed the sex of the patient and the name of the attending physician. By linking to a medical provider database, they could determine the sex of the provider.
The goal was to look at outcomes across four dyads:
- Male patient – male doctor
- Male patient – female doctor
- Female patient – male doctor
- Female patient – female doctor
The primary outcome was 30-day mortality.
I told you that focusing on hospitalists produces some pseudorandomization, but let’s look at the data to be sure. Just under a million patients were treated by approximately 50,000 physicians, 30% of whom were female. And, though female patients and male patients differed, they did not differ with respect to the sex of their hospitalist. So, by physician sex, patients were similar in mean age, race, ethnicity, household income, eligibility for Medicaid, and comorbid conditions. The authors even created a “predicted mortality” score which was similar across the groups as well.
Now, the female physicians were a bit different from the male physicians. The female hospitalists were slightly more likely to have an osteopathic degree, had slightly fewer admissions per year, and were a bit younger.
So, we have broadly similar patients regardless of who their hospitalist was, but hospitalists differ by factors other than their sex. Fine.
I’ve graphed the results here.
This is a relatively small effect, to be sure, but if you multiply it across the millions of hospitalist admissions per year, you can start to put up some real numbers.
So, what is going on here? I see four broad buckets of possibilities.
Let’s start with the obvious explanation: Women, on average, are better doctors than men. I am married to a woman doctor, and based on my personal experience, this explanation is undoubtedly true. But why would that be?
The authors cite data that suggest that female physicians are less likely than male physicians to dismiss patient concerns — and in particular, the concerns of female patients — perhaps leading to fewer missed diagnoses. But this is impossible to measure with administrative data, so this study can no more tell us whether these female hospitalists are more attentive than their male counterparts than it can suggest that the benefit is mediated by the shorter average height of female physicians. Perhaps the key is being closer to the patient?
The second possibility here is that this has nothing to do with the sex of the physician at all; it has to do with those other things that associate with the sex of the physician. We know, for example, that the female physicians saw fewer patients per year than the male physicians, but the study authors adjusted for this in the statistical models. Still, other unmeasured factors (confounders) could be present. By the way, confounders wouldn’t necessarily change the primary finding — you are better off being cared for by female physicians. It’s just not because they are female; it’s a convenient marker for some other quality, such as age.
The third possibility is that the study represents a phenomenon called collider bias. The idea here is that physicians only get into the study if they are hospitalists, and the quality of physicians who choose to become a hospitalist may differ by sex. When deciding on a specialty, a talented resident considering certain lifestyle issues may find hospital medicine particularly attractive — and that draw toward a more lifestyle-friendly specialty may differ by sex, as some prior studies have shown. If true, the pool of women hospitalists may be better than their male counterparts because male physicians of that caliber don’t become hospitalists.
Okay, don’t write in. I’m just trying to cite examples of how to think about collider bias. I can’t prove that this is the case, and in fact the authors do a sensitivity analysis of all physicians, not just hospitalists, and show the same thing. So this is probably not true, but epidemiology is fun, right?
And the fourth possibility: This is nothing but statistical noise. The effect size is incredibly small and just on the border of statistical significance. Especially when you’re working with very large datasets like this, you’ve got to be really careful about overinterpreting statistically significant findings that are nevertheless of small magnitude.
Regardless, it’s an interesting study, one that made me think and, of course, worry a bit about how I would present it. Forgive me if I’ve been indelicate in handling the complex issues of sex, gender, and society here. But I’m not sure what you expect; after all, I’m only a male doctor.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It’s a battle of the sexes today as we dive into a paper that makes you say, “Wow, what an interesting study” and also “Boy, am I glad I didn’t do that study.” That’s because studies like this are always somewhat fraught; they say something about medicine but also something about society — and that makes this a bit precarious. But that’s never stopped us before. So, let’s go ahead and try to answer the question: Do women make better doctors than men?
On the surface, this question seems nearly impossible to answer. It’s too broad; what does it mean to be a “better” doctor? At first blush it seems that there are just too many variables to control for here: the type of doctor, the type of patient, the clinical scenario, and so on.
But this study, “Comparison of hospital mortality and readmission rates by physician and patient sex,” which appears in Annals of Internal Medicine, uses a fairly ingenious method to cut through all the bias by leveraging two simple facts: First, hospital medicine is largely conducted by hospitalists these days; second, due to the shift-based nature of hospitalist work, the hospitalist you get when you are admitted to the hospital is pretty much random.
In other words, if you are admitted to the hospital for an acute illness and get a hospitalist as your attending, you have no control over whether it is a man or a woman. Is this a randomized trial? No, but it’s not bad.
Researchers used Medicare claims data to identify adults over age 65 who had nonelective hospital admissions throughout the United States. The claims revealed the sex of the patient and the name of the attending physician. By linking to a medical provider database, they could determine the sex of the provider.
The goal was to look at outcomes across four dyads:
- Male patient – male doctor
- Male patient – female doctor
- Female patient – male doctor
- Female patient – female doctor
The primary outcome was 30-day mortality.
I told you that focusing on hospitalists produces some pseudorandomization, but let’s look at the data to be sure. Just under a million patients were treated by approximately 50,000 physicians, 30% of whom were female. And, though female patients and male patients differed, they did not differ with respect to the sex of their hospitalist. So, by physician sex, patients were similar in mean age, race, ethnicity, household income, eligibility for Medicaid, and comorbid conditions. The authors even created a “predicted mortality” score which was similar across the groups as well.
Now, the female physicians were a bit different from the male physicians. The female hospitalists were slightly more likely to have an osteopathic degree, had slightly fewer admissions per year, and were a bit younger.
So, we have broadly similar patients regardless of who their hospitalist was, but hospitalists differ by factors other than their sex. Fine.
I’ve graphed the results here.
This is a relatively small effect, to be sure, but if you multiply it across the millions of hospitalist admissions per year, you can start to put up some real numbers.
So, what is going on here? I see four broad buckets of possibilities.
Let’s start with the obvious explanation: Women, on average, are better doctors than men. I am married to a woman doctor, and based on my personal experience, this explanation is undoubtedly true. But why would that be?
The authors cite data that suggest that female physicians are less likely than male physicians to dismiss patient concerns — and in particular, the concerns of female patients — perhaps leading to fewer missed diagnoses. But this is impossible to measure with administrative data, so this study can no more tell us whether these female hospitalists are more attentive than their male counterparts than it can suggest that the benefit is mediated by the shorter average height of female physicians. Perhaps the key is being closer to the patient?
The second possibility here is that this has nothing to do with the sex of the physician at all; it has to do with those other things that associate with the sex of the physician. We know, for example, that the female physicians saw fewer patients per year than the male physicians, but the study authors adjusted for this in the statistical models. Still, other unmeasured factors (confounders) could be present. By the way, confounders wouldn’t necessarily change the primary finding — you are better off being cared for by female physicians. It’s just not because they are female; it’s a convenient marker for some other quality, such as age.
The third possibility is that the study represents a phenomenon called collider bias. The idea here is that physicians only get into the study if they are hospitalists, and the quality of physicians who choose to become a hospitalist may differ by sex. When deciding on a specialty, a talented resident considering certain lifestyle issues may find hospital medicine particularly attractive — and that draw toward a more lifestyle-friendly specialty may differ by sex, as some prior studies have shown. If true, the pool of women hospitalists may be better than their male counterparts because male physicians of that caliber don’t become hospitalists.
Okay, don’t write in. I’m just trying to cite examples of how to think about collider bias. I can’t prove that this is the case, and in fact the authors do a sensitivity analysis of all physicians, not just hospitalists, and show the same thing. So this is probably not true, but epidemiology is fun, right?
And the fourth possibility: This is nothing but statistical noise. The effect size is incredibly small and just on the border of statistical significance. Especially when you’re working with very large datasets like this, you’ve got to be really careful about overinterpreting statistically significant findings that are nevertheless of small magnitude.
Regardless, it’s an interesting study, one that made me think and, of course, worry a bit about how I would present it. Forgive me if I’ve been indelicate in handling the complex issues of sex, gender, and society here. But I’m not sure what you expect; after all, I’m only a male doctor.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Avoidance Predicts Worse Long-term Outcomes From Intensive OCD Treatment
BOSTON — , a new analysis shows.
Although avoidant patients with OCD reported symptom improvement immediately after treatment, baseline avoidance was associated with significantly worse outcomes 1 year later.
“Avoidance is often overlooked in OCD,” said lead investigator Michael Wheaton, PhD, an assistant professor of psychology at Barnard College in New York. “It’s really important clinically to focus on that.”
The findings were presented at the Anxiety and Depression Association of America (ADAA) annual conference and published online in the Journal of Obsessive-Compulsive and Related Disorders.
The Avoidance Question
Although ERP is often included in treatment for OCD, between 38% and 60% of patients have residual symptoms after treatment and as many as a quarter don’t respond at all, Dr. Wheaton said.
Severe pretreatment avoidance could affect the efficacy of ERP, which involves exposing patients to situations and stimuli they may usually avoid. But prior research to identify predictors of ERP outcomes have largely excluded severity of pretreatment avoidance as a factor.
The new study analyzed data from 161 Norwegian adults with treatment-resistant OCD who participated in a concentrated ERP therapy called the Bergen 4-day Exposure and Response Prevention (B4DT) treatment. This method delivers intensive treatment over 4 consecutive days in small groups with a 1:1 ratio of therapists to patients.
B4DT is common throughout Norway, with the treatment offered at 55 clinics, and has been trialed in other countries including the United States, Nepal, Ecuador, and Kenya.
Symptom severity was measured using the Yale-Brown Obsessive Compulsive Scale (YBOCS) at baseline, immediately after treatment, and 3 and 12 months later. Functional impairment was measured 12 months after treatment using the Work and Social Adjustment Scale.
Although the formal scoring of the YBOCS does not include any questions about avoidance, one question in the auxiliary items does: “Have you been avoiding doing anything, going anyplace or being with anyone because of obsessional thoughts or out of a need to perform compulsions?”
Dr. Wheaton used this response, which is rated on a five-point scale, to measure avoidance. Overall, 18.8% of participants had no deliberate avoidance, 15% were rated as having mild avoidance, 36% moderate, 23% severe, and 6.8% extreme.
Long-Term Outcomes
Overall, 84% of participants responded to treatment, with a change in mean YBOCS scores from 26.98 at baseline to 12.28 immediately after treatment. Acute outcomes were similar between avoidant and nonavoidant patients.
But at 12-month follow-up, even after controlling for pretreatment OCD severity, patients with more extensive avoidance at baseline had worse long-term outcomes — both more severe OCD symptoms (P = .031) and greater functional impairment (P = .002).
Across all patients, average avoidance decreased significantly immediately after the concentrated ERP treatment. Average avoidance increased somewhat at 3- and 12-month follow-up but remained significantly improved from pretreatment.
Interestingly, patients’ change in avoidance immediately post-treatment to 3 months post-treatment predicted worsening of OCD severity at 12 months. This change could potentially identify people at risk of relapse, Dr. Wheaton said.
Previous research has shown that pretreatment OCD severity, measured using the YBOCS, does not significantly predict ERP outcomes, and this study found the same.
Relapse Prevention
“The fact that they did equally well in the short run I think was great,” Dr. Wheaton said.
Previous research, including 2018 and 2023 papers from Wheaton’s team, has shown that more avoidant patients have worse outcomes from standard 12-week ERP programs.
One possible explanation for this difference is that in the Bergen treatment, most exposures happen during face-to-face time with a therapist instead of as homework, which may be easier to avoid, he said.
“But then the finding was that their symptoms were worsening over time — their avoidance was sliding back into old habits,” said Dr. Wheaton.
He would like to see the study replicated in diverse populations outside Norway and in treatment-naive people. Dr. Wheaton also noted that the study assessed avoidance with only a single item.
Future work is needed to test ways to improve relapse prevention. For example, clinicians may be able to monitor for avoidance behaviors post-treatment, which could be the start of a relapse, said Dr. Wheaton.
Although clinicians consider avoidance when treating phobias, social anxiety disorder, and panic disorder, “somehow avoidance got relegated to item 11 on the YBOCS that isn’t scored,” Helen Blair Simpson, MD, PhD, director of the Center for OCD and Related Disorders at Columbia University, New York, New York, said during the presentation.
A direct implication of Dr. Wheaton’s findings to clinical practice is to “talk to people about their avoidance right up front,” said Dr. Simpson, who was not part of the study.
Clinicians who deliver ERP in their practices “can apply this tomorrow,” Dr. Simpson added.
Dr. Wheaton reported no disclosures. Dr. Simpson reported a stipend from the American Medical Association for serving as associate editor of JAMA Psychiatry and royalties from UpToDate, Inc for articles on OCD and from Cambridge University Press for editing a book on anxiety disorders.
A version of this article appeared on Medscape.com.
BOSTON — , a new analysis shows.
Although avoidant patients with OCD reported symptom improvement immediately after treatment, baseline avoidance was associated with significantly worse outcomes 1 year later.
“Avoidance is often overlooked in OCD,” said lead investigator Michael Wheaton, PhD, an assistant professor of psychology at Barnard College in New York. “It’s really important clinically to focus on that.”
The findings were presented at the Anxiety and Depression Association of America (ADAA) annual conference and published online in the Journal of Obsessive-Compulsive and Related Disorders.
The Avoidance Question
Although ERP is often included in treatment for OCD, between 38% and 60% of patients have residual symptoms after treatment and as many as a quarter don’t respond at all, Dr. Wheaton said.
Severe pretreatment avoidance could affect the efficacy of ERP, which involves exposing patients to situations and stimuli they may usually avoid. But prior research to identify predictors of ERP outcomes have largely excluded severity of pretreatment avoidance as a factor.
The new study analyzed data from 161 Norwegian adults with treatment-resistant OCD who participated in a concentrated ERP therapy called the Bergen 4-day Exposure and Response Prevention (B4DT) treatment. This method delivers intensive treatment over 4 consecutive days in small groups with a 1:1 ratio of therapists to patients.
B4DT is common throughout Norway, with the treatment offered at 55 clinics, and has been trialed in other countries including the United States, Nepal, Ecuador, and Kenya.
Symptom severity was measured using the Yale-Brown Obsessive Compulsive Scale (YBOCS) at baseline, immediately after treatment, and 3 and 12 months later. Functional impairment was measured 12 months after treatment using the Work and Social Adjustment Scale.
Although the formal scoring of the YBOCS does not include any questions about avoidance, one question in the auxiliary items does: “Have you been avoiding doing anything, going anyplace or being with anyone because of obsessional thoughts or out of a need to perform compulsions?”
Dr. Wheaton used this response, which is rated on a five-point scale, to measure avoidance. Overall, 18.8% of participants had no deliberate avoidance, 15% were rated as having mild avoidance, 36% moderate, 23% severe, and 6.8% extreme.
Long-Term Outcomes
Overall, 84% of participants responded to treatment, with a change in mean YBOCS scores from 26.98 at baseline to 12.28 immediately after treatment. Acute outcomes were similar between avoidant and nonavoidant patients.
But at 12-month follow-up, even after controlling for pretreatment OCD severity, patients with more extensive avoidance at baseline had worse long-term outcomes — both more severe OCD symptoms (P = .031) and greater functional impairment (P = .002).
Across all patients, average avoidance decreased significantly immediately after the concentrated ERP treatment. Average avoidance increased somewhat at 3- and 12-month follow-up but remained significantly improved from pretreatment.
Interestingly, patients’ change in avoidance immediately post-treatment to 3 months post-treatment predicted worsening of OCD severity at 12 months. This change could potentially identify people at risk of relapse, Dr. Wheaton said.
Previous research has shown that pretreatment OCD severity, measured using the YBOCS, does not significantly predict ERP outcomes, and this study found the same.
Relapse Prevention
“The fact that they did equally well in the short run I think was great,” Dr. Wheaton said.
Previous research, including 2018 and 2023 papers from Wheaton’s team, has shown that more avoidant patients have worse outcomes from standard 12-week ERP programs.
One possible explanation for this difference is that in the Bergen treatment, most exposures happen during face-to-face time with a therapist instead of as homework, which may be easier to avoid, he said.
“But then the finding was that their symptoms were worsening over time — their avoidance was sliding back into old habits,” said Dr. Wheaton.
He would like to see the study replicated in diverse populations outside Norway and in treatment-naive people. Dr. Wheaton also noted that the study assessed avoidance with only a single item.
Future work is needed to test ways to improve relapse prevention. For example, clinicians may be able to monitor for avoidance behaviors post-treatment, which could be the start of a relapse, said Dr. Wheaton.
Although clinicians consider avoidance when treating phobias, social anxiety disorder, and panic disorder, “somehow avoidance got relegated to item 11 on the YBOCS that isn’t scored,” Helen Blair Simpson, MD, PhD, director of the Center for OCD and Related Disorders at Columbia University, New York, New York, said during the presentation.
A direct implication of Dr. Wheaton’s findings to clinical practice is to “talk to people about their avoidance right up front,” said Dr. Simpson, who was not part of the study.
Clinicians who deliver ERP in their practices “can apply this tomorrow,” Dr. Simpson added.
Dr. Wheaton reported no disclosures. Dr. Simpson reported a stipend from the American Medical Association for serving as associate editor of JAMA Psychiatry and royalties from UpToDate, Inc for articles on OCD and from Cambridge University Press for editing a book on anxiety disorders.
A version of this article appeared on Medscape.com.
BOSTON — , a new analysis shows.
Although avoidant patients with OCD reported symptom improvement immediately after treatment, baseline avoidance was associated with significantly worse outcomes 1 year later.
“Avoidance is often overlooked in OCD,” said lead investigator Michael Wheaton, PhD, an assistant professor of psychology at Barnard College in New York. “It’s really important clinically to focus on that.”
The findings were presented at the Anxiety and Depression Association of America (ADAA) annual conference and published online in the Journal of Obsessive-Compulsive and Related Disorders.
The Avoidance Question
Although ERP is often included in treatment for OCD, between 38% and 60% of patients have residual symptoms after treatment and as many as a quarter don’t respond at all, Dr. Wheaton said.
Severe pretreatment avoidance could affect the efficacy of ERP, which involves exposing patients to situations and stimuli they may usually avoid. But prior research to identify predictors of ERP outcomes have largely excluded severity of pretreatment avoidance as a factor.
The new study analyzed data from 161 Norwegian adults with treatment-resistant OCD who participated in a concentrated ERP therapy called the Bergen 4-day Exposure and Response Prevention (B4DT) treatment. This method delivers intensive treatment over 4 consecutive days in small groups with a 1:1 ratio of therapists to patients.
B4DT is common throughout Norway, with the treatment offered at 55 clinics, and has been trialed in other countries including the United States, Nepal, Ecuador, and Kenya.
Symptom severity was measured using the Yale-Brown Obsessive Compulsive Scale (YBOCS) at baseline, immediately after treatment, and 3 and 12 months later. Functional impairment was measured 12 months after treatment using the Work and Social Adjustment Scale.
Although the formal scoring of the YBOCS does not include any questions about avoidance, one question in the auxiliary items does: “Have you been avoiding doing anything, going anyplace or being with anyone because of obsessional thoughts or out of a need to perform compulsions?”
Dr. Wheaton used this response, which is rated on a five-point scale, to measure avoidance. Overall, 18.8% of participants had no deliberate avoidance, 15% were rated as having mild avoidance, 36% moderate, 23% severe, and 6.8% extreme.
Long-Term Outcomes
Overall, 84% of participants responded to treatment, with a change in mean YBOCS scores from 26.98 at baseline to 12.28 immediately after treatment. Acute outcomes were similar between avoidant and nonavoidant patients.
But at 12-month follow-up, even after controlling for pretreatment OCD severity, patients with more extensive avoidance at baseline had worse long-term outcomes — both more severe OCD symptoms (P = .031) and greater functional impairment (P = .002).
Across all patients, average avoidance decreased significantly immediately after the concentrated ERP treatment. Average avoidance increased somewhat at 3- and 12-month follow-up but remained significantly improved from pretreatment.
Interestingly, patients’ change in avoidance immediately post-treatment to 3 months post-treatment predicted worsening of OCD severity at 12 months. This change could potentially identify people at risk of relapse, Dr. Wheaton said.
Previous research has shown that pretreatment OCD severity, measured using the YBOCS, does not significantly predict ERP outcomes, and this study found the same.
Relapse Prevention
“The fact that they did equally well in the short run I think was great,” Dr. Wheaton said.
Previous research, including 2018 and 2023 papers from Wheaton’s team, has shown that more avoidant patients have worse outcomes from standard 12-week ERP programs.
One possible explanation for this difference is that in the Bergen treatment, most exposures happen during face-to-face time with a therapist instead of as homework, which may be easier to avoid, he said.
“But then the finding was that their symptoms were worsening over time — their avoidance was sliding back into old habits,” said Dr. Wheaton.
He would like to see the study replicated in diverse populations outside Norway and in treatment-naive people. Dr. Wheaton also noted that the study assessed avoidance with only a single item.
Future work is needed to test ways to improve relapse prevention. For example, clinicians may be able to monitor for avoidance behaviors post-treatment, which could be the start of a relapse, said Dr. Wheaton.
Although clinicians consider avoidance when treating phobias, social anxiety disorder, and panic disorder, “somehow avoidance got relegated to item 11 on the YBOCS that isn’t scored,” Helen Blair Simpson, MD, PhD, director of the Center for OCD and Related Disorders at Columbia University, New York, New York, said during the presentation.
A direct implication of Dr. Wheaton’s findings to clinical practice is to “talk to people about their avoidance right up front,” said Dr. Simpson, who was not part of the study.
Clinicians who deliver ERP in their practices “can apply this tomorrow,” Dr. Simpson added.
Dr. Wheaton reported no disclosures. Dr. Simpson reported a stipend from the American Medical Association for serving as associate editor of JAMA Psychiatry and royalties from UpToDate, Inc for articles on OCD and from Cambridge University Press for editing a book on anxiety disorders.
A version of this article appeared on Medscape.com.
FROM ADAA 2024
Menopause, RSV, and More: 4 New Meds to Know
BOSTON — The US Food and Drug Administration (FDA) approved 55 new medications in 2023 and 11 more in 2024 to date.
A New First-Line for GERD?
Vonoprazan, an oral potassium-competitive acid blocker — which received FDA approval in November 2023 — may be a good alternative for patients whose symptoms continue to linger despite taking medications designated to treat gastroesophageal reflux disease (GERD).
GERD is the most common gastrointestinal symptom encountered by primary care physicians. Proton-pump inhibitors (PPIs) are the first-line treatment for the condition but can have long-term side effects such as Clostridioides difficile infection and kidney lesions.
“We know that not all patients are going to have symptom relief with H2 blockers and PPIs, so there’s an opportunity for patients who don’t get full symptom relief,” Dr. Smetana told attendees.
Vonoprazan blocks potassium binding to ATPase proton pumps and inhibits the secretion of gastric acid.
The approval of vonoprazan for erosive GERD was based on results from the phase 3 PHALCON-EE study, a randomized, double-blind, multicenter study that found the drug to be more effective than lansoprazole in treating erosive esophagitis.
Vonoprazan “has more rapid absorption than PPIs [and a] longer half-life and is more potent than PPIs, so theoretically it could be more effective in certain settings,” Dr. Smetana said.
Vonoprazan is FDA approved for only 6 months of use. Despite its efficacy, cost may be a barrier to many patients. H2 blockers generally cost patients less than $10 for 1 month’s supply, whereas vonoprazan can cost up to $650.
Nonhormonal Drug for Menopause
Fezolinetant, the first neurokinin receptor antagonist to receive approval from the FDA to treat vasomotor symptoms, may be an option for women concerned about hormone-based therapy for menopausal hot flashes.
“[Fezolinetant] specifically works in the area of the brain that’s involved in body temperature regulation and sweating,” Dr. Smetana said.
Results from the SKYLIGHT 1 randomized controlled trial of fezolinetant found the medication reduced the frequency and severity of hot flashes. Some of the side effects include abdominal pain, diarrhea, and insomnia.
Other nonestrogen treatments, including selective serotonin reuptake inhibitors (SSRIs), gabapentin, cognitive-behavioral therapy, and hypnosis, are modestly effective, according to the North American Menopause Society.
“[Fezolinetant] offers a different option that physicians may be more comfortable prescribing,” Dr. Smetana said. “And I think this will be an important addition to nonhormonal therapy.”
RSV Vaccine for Everyone
Once considered an illness that is more prevalent in young children, respiratory syncytial virus (RSV) has become more prevalent and severe among older adults. Between 60,000 and 120,000 older adults are hospitalized and 6000-10,000 die of RSV infection each year, according to the US Centers for Disease Control and Prevention.
The FDA has approved two RSV vaccines approved for older adults, but clinicians may find it challenging to get older patients vaccinated for this and other preventable illnesses.
Patients who received the RSV vaccine had an 83% relative risk reduction for the illness, according to a recent study, and an overall lower risk for hospitalization.
Moderna is developing an mRNA vaccine for RSV that is similar to many COVID-19 vaccines. A study published in 2023 in The New England Journal of Medicine found no cases of neuroinflammatory disorders among patients who received the mRNA RSV vaccine, with a median follow-up of 112 days.
“This is important given ongoing concerns of neurological safety,” among older adults who receive the RSV vaccine, Dr. Smetana said.
As of March 2024, the CDC recommends shared decision-making for adults older than 60 years and for healthcare providers to “consider” rather than “recommend” the vaccine for their patients. The agency’s Adult RSV Work Group plans to meet at June 2024 to reconsider whether shared clinical decision-making remains the preferred policy option.
New Antidepressants
A medication thrice rejected by the FDA is now heading a new class of drugs to treat major depressive disorder.
Gepirone, a 5-HT1A receptor agonist, has a different mechanism of action from that of SSRIs, which are currently considered the first-line treatment for depression.
Gepirone was rejected by the FDA in 2002, 2004, and 2007, with concerns that the efficacy studies were too small. In 2015, an FDA advisory committee agreed that the evidence to date did not support approval of an extended-release form of the drug. But the agency decided to approve the medication in September 2023.
“So why is this medication worth discussing now?” Dr. Smetana said. “It’s because the side effect profile is different from existing antidepressants.”
Many patients may stop using SSRIs because of side effects such as insomnia and loss of libido, Dr. Smetana said. Gepirone has the potential to avoid activation of other 5-HT receptors that mediate side effects, he said.
Studies suggest that gepirone reduces both anxiety and depression scores on the Hamilton Depression Rating Scale in patients who have both conditions and decreases rates of depression relapse compared with placebo through at least 48 weeks. The drug also may be less likely than SSRIs to cause sexual dysfunction in men, Dr. Smetana said.
Gepirone will be available to prescribe to patients in fall 2024.
Dr. Smetana reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
BOSTON — The US Food and Drug Administration (FDA) approved 55 new medications in 2023 and 11 more in 2024 to date.
A New First-Line for GERD?
Vonoprazan, an oral potassium-competitive acid blocker — which received FDA approval in November 2023 — may be a good alternative for patients whose symptoms continue to linger despite taking medications designated to treat gastroesophageal reflux disease (GERD).
GERD is the most common gastrointestinal symptom encountered by primary care physicians. Proton-pump inhibitors (PPIs) are the first-line treatment for the condition but can have long-term side effects such as Clostridioides difficile infection and kidney lesions.
“We know that not all patients are going to have symptom relief with H2 blockers and PPIs, so there’s an opportunity for patients who don’t get full symptom relief,” Dr. Smetana told attendees.
Vonoprazan blocks potassium binding to ATPase proton pumps and inhibits the secretion of gastric acid.
The approval of vonoprazan for erosive GERD was based on results from the phase 3 PHALCON-EE study, a randomized, double-blind, multicenter study that found the drug to be more effective than lansoprazole in treating erosive esophagitis.
Vonoprazan “has more rapid absorption than PPIs [and a] longer half-life and is more potent than PPIs, so theoretically it could be more effective in certain settings,” Dr. Smetana said.
Vonoprazan is FDA approved for only 6 months of use. Despite its efficacy, cost may be a barrier to many patients. H2 blockers generally cost patients less than $10 for 1 month’s supply, whereas vonoprazan can cost up to $650.
Nonhormonal Drug for Menopause
Fezolinetant, the first neurokinin receptor antagonist to receive approval from the FDA to treat vasomotor symptoms, may be an option for women concerned about hormone-based therapy for menopausal hot flashes.
“[Fezolinetant] specifically works in the area of the brain that’s involved in body temperature regulation and sweating,” Dr. Smetana said.
Results from the SKYLIGHT 1 randomized controlled trial of fezolinetant found the medication reduced the frequency and severity of hot flashes. Some of the side effects include abdominal pain, diarrhea, and insomnia.
Other nonestrogen treatments, including selective serotonin reuptake inhibitors (SSRIs), gabapentin, cognitive-behavioral therapy, and hypnosis, are modestly effective, according to the North American Menopause Society.
“[Fezolinetant] offers a different option that physicians may be more comfortable prescribing,” Dr. Smetana said. “And I think this will be an important addition to nonhormonal therapy.”
RSV Vaccine for Everyone
Once considered an illness that is more prevalent in young children, respiratory syncytial virus (RSV) has become more prevalent and severe among older adults. Between 60,000 and 120,000 older adults are hospitalized and 6000-10,000 die of RSV infection each year, according to the US Centers for Disease Control and Prevention.
The FDA has approved two RSV vaccines approved for older adults, but clinicians may find it challenging to get older patients vaccinated for this and other preventable illnesses.
Patients who received the RSV vaccine had an 83% relative risk reduction for the illness, according to a recent study, and an overall lower risk for hospitalization.
Moderna is developing an mRNA vaccine for RSV that is similar to many COVID-19 vaccines. A study published in 2023 in The New England Journal of Medicine found no cases of neuroinflammatory disorders among patients who received the mRNA RSV vaccine, with a median follow-up of 112 days.
“This is important given ongoing concerns of neurological safety,” among older adults who receive the RSV vaccine, Dr. Smetana said.
As of March 2024, the CDC recommends shared decision-making for adults older than 60 years and for healthcare providers to “consider” rather than “recommend” the vaccine for their patients. The agency’s Adult RSV Work Group plans to meet at June 2024 to reconsider whether shared clinical decision-making remains the preferred policy option.
New Antidepressants
A medication thrice rejected by the FDA is now heading a new class of drugs to treat major depressive disorder.
Gepirone, a 5-HT1A receptor agonist, has a different mechanism of action from that of SSRIs, which are currently considered the first-line treatment for depression.
Gepirone was rejected by the FDA in 2002, 2004, and 2007, with concerns that the efficacy studies were too small. In 2015, an FDA advisory committee agreed that the evidence to date did not support approval of an extended-release form of the drug. But the agency decided to approve the medication in September 2023.
“So why is this medication worth discussing now?” Dr. Smetana said. “It’s because the side effect profile is different from existing antidepressants.”
Many patients may stop using SSRIs because of side effects such as insomnia and loss of libido, Dr. Smetana said. Gepirone has the potential to avoid activation of other 5-HT receptors that mediate side effects, he said.
Studies suggest that gepirone reduces both anxiety and depression scores on the Hamilton Depression Rating Scale in patients who have both conditions and decreases rates of depression relapse compared with placebo through at least 48 weeks. The drug also may be less likely than SSRIs to cause sexual dysfunction in men, Dr. Smetana said.
Gepirone will be available to prescribe to patients in fall 2024.
Dr. Smetana reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
BOSTON — The US Food and Drug Administration (FDA) approved 55 new medications in 2023 and 11 more in 2024 to date.
A New First-Line for GERD?
Vonoprazan, an oral potassium-competitive acid blocker — which received FDA approval in November 2023 — may be a good alternative for patients whose symptoms continue to linger despite taking medications designated to treat gastroesophageal reflux disease (GERD).
GERD is the most common gastrointestinal symptom encountered by primary care physicians. Proton-pump inhibitors (PPIs) are the first-line treatment for the condition but can have long-term side effects such as Clostridioides difficile infection and kidney lesions.
“We know that not all patients are going to have symptom relief with H2 blockers and PPIs, so there’s an opportunity for patients who don’t get full symptom relief,” Dr. Smetana told attendees.
Vonoprazan blocks potassium binding to ATPase proton pumps and inhibits the secretion of gastric acid.
The approval of vonoprazan for erosive GERD was based on results from the phase 3 PHALCON-EE study, a randomized, double-blind, multicenter study that found the drug to be more effective than lansoprazole in treating erosive esophagitis.
Vonoprazan “has more rapid absorption than PPIs [and a] longer half-life and is more potent than PPIs, so theoretically it could be more effective in certain settings,” Dr. Smetana said.
Vonoprazan is FDA approved for only 6 months of use. Despite its efficacy, cost may be a barrier to many patients. H2 blockers generally cost patients less than $10 for 1 month’s supply, whereas vonoprazan can cost up to $650.
Nonhormonal Drug for Menopause
Fezolinetant, the first neurokinin receptor antagonist to receive approval from the FDA to treat vasomotor symptoms, may be an option for women concerned about hormone-based therapy for menopausal hot flashes.
“[Fezolinetant] specifically works in the area of the brain that’s involved in body temperature regulation and sweating,” Dr. Smetana said.
Results from the SKYLIGHT 1 randomized controlled trial of fezolinetant found the medication reduced the frequency and severity of hot flashes. Some of the side effects include abdominal pain, diarrhea, and insomnia.
Other nonestrogen treatments, including selective serotonin reuptake inhibitors (SSRIs), gabapentin, cognitive-behavioral therapy, and hypnosis, are modestly effective, according to the North American Menopause Society.
“[Fezolinetant] offers a different option that physicians may be more comfortable prescribing,” Dr. Smetana said. “And I think this will be an important addition to nonhormonal therapy.”
RSV Vaccine for Everyone
Once considered an illness that is more prevalent in young children, respiratory syncytial virus (RSV) has become more prevalent and severe among older adults. Between 60,000 and 120,000 older adults are hospitalized and 6000-10,000 die of RSV infection each year, according to the US Centers for Disease Control and Prevention.
The FDA has approved two RSV vaccines approved for older adults, but clinicians may find it challenging to get older patients vaccinated for this and other preventable illnesses.
Patients who received the RSV vaccine had an 83% relative risk reduction for the illness, according to a recent study, and an overall lower risk for hospitalization.
Moderna is developing an mRNA vaccine for RSV that is similar to many COVID-19 vaccines. A study published in 2023 in The New England Journal of Medicine found no cases of neuroinflammatory disorders among patients who received the mRNA RSV vaccine, with a median follow-up of 112 days.
“This is important given ongoing concerns of neurological safety,” among older adults who receive the RSV vaccine, Dr. Smetana said.
As of March 2024, the CDC recommends shared decision-making for adults older than 60 years and for healthcare providers to “consider” rather than “recommend” the vaccine for their patients. The agency’s Adult RSV Work Group plans to meet at June 2024 to reconsider whether shared clinical decision-making remains the preferred policy option.
New Antidepressants
A medication thrice rejected by the FDA is now heading a new class of drugs to treat major depressive disorder.
Gepirone, a 5-HT1A receptor agonist, has a different mechanism of action from that of SSRIs, which are currently considered the first-line treatment for depression.
Gepirone was rejected by the FDA in 2002, 2004, and 2007, with concerns that the efficacy studies were too small. In 2015, an FDA advisory committee agreed that the evidence to date did not support approval of an extended-release form of the drug. But the agency decided to approve the medication in September 2023.
“So why is this medication worth discussing now?” Dr. Smetana said. “It’s because the side effect profile is different from existing antidepressants.”
Many patients may stop using SSRIs because of side effects such as insomnia and loss of libido, Dr. Smetana said. Gepirone has the potential to avoid activation of other 5-HT receptors that mediate side effects, he said.
Studies suggest that gepirone reduces both anxiety and depression scores on the Hamilton Depression Rating Scale in patients who have both conditions and decreases rates of depression relapse compared with placebo through at least 48 weeks. The drug also may be less likely than SSRIs to cause sexual dysfunction in men, Dr. Smetana said.
Gepirone will be available to prescribe to patients in fall 2024.
Dr. Smetana reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
Adding Life to Your Patients’ Years
Caring for older adults was one of the most rewarding parts of my years practicing as a clinical cardiologist. I appreciated their wisdom, humor, and, very often, their respect and appreciation for physicians. It was always upsetting to see them suffer a mild fall or episode of atrial fibrillation and recognize that it could have major health ramifications.
That is not just a question for geriatric care. With fewer than two practicing geriatricians for every 10,000 older individuals, it is obvious that geriatricians cannot shoulder this responsibility alone. Almost all primary care physicians and subspecialists should prepare to care for older individuals and help them age healthfully.
Susan Friedman, MD, a board-certified geriatrics and lifestyle medicine clinician at the University of Rochester School of Medicine and Dentistry, Rochester, New York, reviewed the literature on the connection between lifestyle and healthy aging and concluded that the integration of lifestyle medicine into medical care for older adults is key to compressing morbidity. The pillars of lifestyle medicine — optimal nutrition, physical activity, stress management, restorative sleep, positive social connections, and avoidance of risky substances — both individually or as a sum are associated with less chronic disease, improved engagement in life, better physical and cognitive function, less frailty, and less sarcopenia. Framing discussions with patients around the six pillars of lifestyle medicine can be an effective strategy.
Optimal Nutrition
For a variety of reasons, older adults, especially those living alone, often lose the desire to prepare a nourishing meal. Older adults require different protein intake than younger patients to offset age-related sarcopenia, but helping them select healthy sources of protein is imperative. Both adequate protein consumption and eating patterns high in vegetables, legumes, fruit, and nuts and low in saturated fat, red meat, and processed meat can lower the risk of developing frailty.
Asking a patient to share a 24-hour food recall, and based upon that, resourcing nutritional guidance, a lifestyle medicine program or specialist, and insurance or community resources for food-as-medicine services, is a good first step.
Physical Activity
Increasing general physical activity can be a tough ask for many older adults, and joint pain is a common reason they demur. Messaging around targeted exercises to mitigate falls, improve muscle strength, and reduce joint pain may be more appealing. Contemporary research demonstrates that exercise, particularly open-skill exercise that requires quick decisions (such as table tennis) can be powerful. Maintaining cognition, mood enhancement, and independence may also be motivating messages.
The first step is curiosity: What does your patient like to do? Referral to a physical therapist or an exercise specialist to provide stepwise guidance along with resourcing community opportunities can then follow.
Restorative Sleep
“I’m old. I don’t need as much sleep.” We’ve probably all heard older patients say this. But the National Sleep Foundation’s report on sleep health and aging indicates that the need to sleep does not decrease with age. The ability to sleep, however, may decline. Assessing and treating disordered sleep is another example of how each lifestyle medicine pillar, such as nutrition and physical activity, is multidimensional and interacts to support the functional integrity of older patients. It’s hard to feel motivated to go for a walk if you lack adequate sleep.
Stress Management
Exploring stress with patients can be very revealing. Do they experience stress that energizes and has a positive effect? How much of their day is spent in negatively impactful distress? Chronic stress has been shown to affect immune function in older individuals. Start conversations with your older patients to normalize the importance of stress as a health measure.
Positive Social Connections
Loneliness puts individuals at higher risk for heart disease, stroke, and dementia and even increases the risk for premature death by up to 60%. Yet, clinicians and patients rarely discuss social connections during medical appointments. Tools such as the UCLA Loneliness Scale exist for health practitioners to assess and identify patients at risk for loneliness, as do resources to integrate social care into the delivery of healthcare.
Avoidance of Risky Substances
Alcohol assessments are not just for younger patients. One study found that 5.6 million adults ages 65 or older engaged in binge drinking in the past month. Because of body changes, the negative effects of alcohol may be greater on older adults, including interactions between alcohol and commonly prescribed medications.
Conducting a lifestyle assessment is an important way to engage with older patients and allows clinicians to identify opportunities to improve health behaviors, understand obstacles, and support patients to make lifestyle changes. It may uncover ways to remove some of the pill and treatment burdens that older adults often experience. The American College of Lifestyle Medicine (ACLM) offers clinical practice resources to support clinicians as well as “Lifestyle Medicine and Food as Medicine Essentials,” a 5.5-hour complimentary CE/CME course on food and lifestyle medicine that introduces clinicians to the therapeutic use of lifestyle medicine. ACLM also offers members interest groups focused on geriatrics, fitness, and mental health, which may be beneficial to clinicians treating older adults.
By engaging with older patients on their lifestyle behaviors, we can ensure that we are doing all we can to help them live longer — and live better.
Dr. Collings is director of lifestyle medicine, Silicon Valley Medical Development, and past president, American College of Lifestyle Medicine, Mountain View, California. She has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Caring for older adults was one of the most rewarding parts of my years practicing as a clinical cardiologist. I appreciated their wisdom, humor, and, very often, their respect and appreciation for physicians. It was always upsetting to see them suffer a mild fall or episode of atrial fibrillation and recognize that it could have major health ramifications.
That is not just a question for geriatric care. With fewer than two practicing geriatricians for every 10,000 older individuals, it is obvious that geriatricians cannot shoulder this responsibility alone. Almost all primary care physicians and subspecialists should prepare to care for older individuals and help them age healthfully.
Susan Friedman, MD, a board-certified geriatrics and lifestyle medicine clinician at the University of Rochester School of Medicine and Dentistry, Rochester, New York, reviewed the literature on the connection between lifestyle and healthy aging and concluded that the integration of lifestyle medicine into medical care for older adults is key to compressing morbidity. The pillars of lifestyle medicine — optimal nutrition, physical activity, stress management, restorative sleep, positive social connections, and avoidance of risky substances — both individually or as a sum are associated with less chronic disease, improved engagement in life, better physical and cognitive function, less frailty, and less sarcopenia. Framing discussions with patients around the six pillars of lifestyle medicine can be an effective strategy.
Optimal Nutrition
For a variety of reasons, older adults, especially those living alone, often lose the desire to prepare a nourishing meal. Older adults require different protein intake than younger patients to offset age-related sarcopenia, but helping them select healthy sources of protein is imperative. Both adequate protein consumption and eating patterns high in vegetables, legumes, fruit, and nuts and low in saturated fat, red meat, and processed meat can lower the risk of developing frailty.
Asking a patient to share a 24-hour food recall, and based upon that, resourcing nutritional guidance, a lifestyle medicine program or specialist, and insurance or community resources for food-as-medicine services, is a good first step.
Physical Activity
Increasing general physical activity can be a tough ask for many older adults, and joint pain is a common reason they demur. Messaging around targeted exercises to mitigate falls, improve muscle strength, and reduce joint pain may be more appealing. Contemporary research demonstrates that exercise, particularly open-skill exercise that requires quick decisions (such as table tennis) can be powerful. Maintaining cognition, mood enhancement, and independence may also be motivating messages.
The first step is curiosity: What does your patient like to do? Referral to a physical therapist or an exercise specialist to provide stepwise guidance along with resourcing community opportunities can then follow.
Restorative Sleep
“I’m old. I don’t need as much sleep.” We’ve probably all heard older patients say this. But the National Sleep Foundation’s report on sleep health and aging indicates that the need to sleep does not decrease with age. The ability to sleep, however, may decline. Assessing and treating disordered sleep is another example of how each lifestyle medicine pillar, such as nutrition and physical activity, is multidimensional and interacts to support the functional integrity of older patients. It’s hard to feel motivated to go for a walk if you lack adequate sleep.
Stress Management
Exploring stress with patients can be very revealing. Do they experience stress that energizes and has a positive effect? How much of their day is spent in negatively impactful distress? Chronic stress has been shown to affect immune function in older individuals. Start conversations with your older patients to normalize the importance of stress as a health measure.
Positive Social Connections
Loneliness puts individuals at higher risk for heart disease, stroke, and dementia and even increases the risk for premature death by up to 60%. Yet, clinicians and patients rarely discuss social connections during medical appointments. Tools such as the UCLA Loneliness Scale exist for health practitioners to assess and identify patients at risk for loneliness, as do resources to integrate social care into the delivery of healthcare.
Avoidance of Risky Substances
Alcohol assessments are not just for younger patients. One study found that 5.6 million adults ages 65 or older engaged in binge drinking in the past month. Because of body changes, the negative effects of alcohol may be greater on older adults, including interactions between alcohol and commonly prescribed medications.
Conducting a lifestyle assessment is an important way to engage with older patients and allows clinicians to identify opportunities to improve health behaviors, understand obstacles, and support patients to make lifestyle changes. It may uncover ways to remove some of the pill and treatment burdens that older adults often experience. The American College of Lifestyle Medicine (ACLM) offers clinical practice resources to support clinicians as well as “Lifestyle Medicine and Food as Medicine Essentials,” a 5.5-hour complimentary CE/CME course on food and lifestyle medicine that introduces clinicians to the therapeutic use of lifestyle medicine. ACLM also offers members interest groups focused on geriatrics, fitness, and mental health, which may be beneficial to clinicians treating older adults.
By engaging with older patients on their lifestyle behaviors, we can ensure that we are doing all we can to help them live longer — and live better.
Dr. Collings is director of lifestyle medicine, Silicon Valley Medical Development, and past president, American College of Lifestyle Medicine, Mountain View, California. She has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Caring for older adults was one of the most rewarding parts of my years practicing as a clinical cardiologist. I appreciated their wisdom, humor, and, very often, their respect and appreciation for physicians. It was always upsetting to see them suffer a mild fall or episode of atrial fibrillation and recognize that it could have major health ramifications.
That is not just a question for geriatric care. With fewer than two practicing geriatricians for every 10,000 older individuals, it is obvious that geriatricians cannot shoulder this responsibility alone. Almost all primary care physicians and subspecialists should prepare to care for older individuals and help them age healthfully.
Susan Friedman, MD, a board-certified geriatrics and lifestyle medicine clinician at the University of Rochester School of Medicine and Dentistry, Rochester, New York, reviewed the literature on the connection between lifestyle and healthy aging and concluded that the integration of lifestyle medicine into medical care for older adults is key to compressing morbidity. The pillars of lifestyle medicine — optimal nutrition, physical activity, stress management, restorative sleep, positive social connections, and avoidance of risky substances — both individually or as a sum are associated with less chronic disease, improved engagement in life, better physical and cognitive function, less frailty, and less sarcopenia. Framing discussions with patients around the six pillars of lifestyle medicine can be an effective strategy.
Optimal Nutrition
For a variety of reasons, older adults, especially those living alone, often lose the desire to prepare a nourishing meal. Older adults require different protein intake than younger patients to offset age-related sarcopenia, but helping them select healthy sources of protein is imperative. Both adequate protein consumption and eating patterns high in vegetables, legumes, fruit, and nuts and low in saturated fat, red meat, and processed meat can lower the risk of developing frailty.
Asking a patient to share a 24-hour food recall, and based upon that, resourcing nutritional guidance, a lifestyle medicine program or specialist, and insurance or community resources for food-as-medicine services, is a good first step.
Physical Activity
Increasing general physical activity can be a tough ask for many older adults, and joint pain is a common reason they demur. Messaging around targeted exercises to mitigate falls, improve muscle strength, and reduce joint pain may be more appealing. Contemporary research demonstrates that exercise, particularly open-skill exercise that requires quick decisions (such as table tennis) can be powerful. Maintaining cognition, mood enhancement, and independence may also be motivating messages.
The first step is curiosity: What does your patient like to do? Referral to a physical therapist or an exercise specialist to provide stepwise guidance along with resourcing community opportunities can then follow.
Restorative Sleep
“I’m old. I don’t need as much sleep.” We’ve probably all heard older patients say this. But the National Sleep Foundation’s report on sleep health and aging indicates that the need to sleep does not decrease with age. The ability to sleep, however, may decline. Assessing and treating disordered sleep is another example of how each lifestyle medicine pillar, such as nutrition and physical activity, is multidimensional and interacts to support the functional integrity of older patients. It’s hard to feel motivated to go for a walk if you lack adequate sleep.
Stress Management
Exploring stress with patients can be very revealing. Do they experience stress that energizes and has a positive effect? How much of their day is spent in negatively impactful distress? Chronic stress has been shown to affect immune function in older individuals. Start conversations with your older patients to normalize the importance of stress as a health measure.
Positive Social Connections
Loneliness puts individuals at higher risk for heart disease, stroke, and dementia and even increases the risk for premature death by up to 60%. Yet, clinicians and patients rarely discuss social connections during medical appointments. Tools such as the UCLA Loneliness Scale exist for health practitioners to assess and identify patients at risk for loneliness, as do resources to integrate social care into the delivery of healthcare.
Avoidance of Risky Substances
Alcohol assessments are not just for younger patients. One study found that 5.6 million adults ages 65 or older engaged in binge drinking in the past month. Because of body changes, the negative effects of alcohol may be greater on older adults, including interactions between alcohol and commonly prescribed medications.
Conducting a lifestyle assessment is an important way to engage with older patients and allows clinicians to identify opportunities to improve health behaviors, understand obstacles, and support patients to make lifestyle changes. It may uncover ways to remove some of the pill and treatment burdens that older adults often experience. The American College of Lifestyle Medicine (ACLM) offers clinical practice resources to support clinicians as well as “Lifestyle Medicine and Food as Medicine Essentials,” a 5.5-hour complimentary CE/CME course on food and lifestyle medicine that introduces clinicians to the therapeutic use of lifestyle medicine. ACLM also offers members interest groups focused on geriatrics, fitness, and mental health, which may be beneficial to clinicians treating older adults.
By engaging with older patients on their lifestyle behaviors, we can ensure that we are doing all we can to help them live longer — and live better.
Dr. Collings is director of lifestyle medicine, Silicon Valley Medical Development, and past president, American College of Lifestyle Medicine, Mountain View, California. She has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
How to Play Like a Masters Champ
You know what the happiest animal in the world is? A goldfish. You know why? It’s got a 10-second memory. Be a goldfish. — Ted Lasso
I don’t play much golf. When I do, it’s when my dad is in town. He shoots his age (78). I shoot double mine (52). He was recently here. We played and watched the Masters where he pointed out how I looked a lot like Scottie Scheffler, the now two-time Masters champion. On the 10th hole of his third round, you could see the resemblance. Scheffler’s third shot flew past the hole into the galley. He rifled the fourth past the hole on its way back toward the fairway. It was now a good distance further from the cup than a minute ago. He proceeded to misread his bogey putt, ending his misery with a double bogey. Scheffler went on to bogey the next hole and dropped from first on the leaderboard to fifth. Yes, I looked just like that on my last round. But here is where Scheffler and I differ. After a hole like that, I’d have been apoplectic, seething with self loathing. Scheffler was not. He kept moving. Head up, he sauntered to the next hole as if he had no awareness of what just transpired.
The ability to compartmentalize is useful not only to become the Masters champion, but also to become master of your day. In this way, golf is a nice approximation for life. The best golfers in the world will always have horrible shots and dreadful holes. The winning ones are often those who recover rather than continue in a downward spiral of one bad shot after another.

It’s easy to think of regular days that went just like Scheffler’s atrocious 10th hole. Getting pimped in front of distinguished faculty at Grand Rounds and whiffing (it was Sweet Syndrome). Calling a patient to let him know that his syphilis test did in fact come back positive (it was his father on the phone, also Mr. Rodham). Arguing with a patient that a biopsy was not needed for me to diagnose her with zoster (you’ve lost once, you’ve lost your temper). Each of these made me feel like slamming my club down, quitting the round right then and there. Losing control though, leads to flubbing the next question or arguing with the following patient. The masters let it go. Like goldfish, they live in the present without any thought of what happened 10 seconds ago.

We don’t have to take advice just from Ted Lasso here; there is plenty of research to support this concept of the critical relationship between resilience and psychological flexibility. Specifically, flexible cognitive control allows us to guide attention and to choose appropriate appraisal and good coping strategies. Ultimately, this leads to better performance. You might be a skilled athlete or presenter, but if you can’t regulate your emotions and something goes wrong, then you’ll perform as poorly as an amateur.
Scheffler went on to eagle the 13th hole on that round. He eventually won the 2024 Masters Tournament. Remember that the next time you find yourself in a day that feels like it is spiraling toward disaster. Close the door on the compartment that was the last miserable hole and saunter to the next patient like it never happened.
And maybe close the clubface a bit on address for your next drive.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on X. Write to him at dermnews@mdedge.com.
You know what the happiest animal in the world is? A goldfish. You know why? It’s got a 10-second memory. Be a goldfish. — Ted Lasso
I don’t play much golf. When I do, it’s when my dad is in town. He shoots his age (78). I shoot double mine (52). He was recently here. We played and watched the Masters where he pointed out how I looked a lot like Scottie Scheffler, the now two-time Masters champion. On the 10th hole of his third round, you could see the resemblance. Scheffler’s third shot flew past the hole into the galley. He rifled the fourth past the hole on its way back toward the fairway. It was now a good distance further from the cup than a minute ago. He proceeded to misread his bogey putt, ending his misery with a double bogey. Scheffler went on to bogey the next hole and dropped from first on the leaderboard to fifth. Yes, I looked just like that on my last round. But here is where Scheffler and I differ. After a hole like that, I’d have been apoplectic, seething with self loathing. Scheffler was not. He kept moving. Head up, he sauntered to the next hole as if he had no awareness of what just transpired.
The ability to compartmentalize is useful not only to become the Masters champion, but also to become master of your day. In this way, golf is a nice approximation for life. The best golfers in the world will always have horrible shots and dreadful holes. The winning ones are often those who recover rather than continue in a downward spiral of one bad shot after another.
It’s easy to think of regular days that went just like Scheffler’s atrocious 10th hole. Getting pimped in front of distinguished faculty at Grand Rounds and whiffing (it was Sweet Syndrome). Calling a patient to let him know that his syphilis test did in fact come back positive (it was his father on the phone, also Mr. Rodham). Arguing with a patient that a biopsy was not needed for me to diagnose her with zoster (you’ve lost once, you’ve lost your temper). Each of these made me feel like slamming my club down, quitting the round right then and there. Losing control though, leads to flubbing the next question or arguing with the following patient. The masters let it go. Like goldfish, they live in the present without any thought of what happened 10 seconds ago.
We don’t have to take advice just from Ted Lasso here; there is plenty of research to support this concept of the critical relationship between resilience and psychological flexibility. Specifically, flexible cognitive control allows us to guide attention and to choose appropriate appraisal and good coping strategies. Ultimately, this leads to better performance. You might be a skilled athlete or presenter, but if you can’t regulate your emotions and something goes wrong, then you’ll perform as poorly as an amateur.
Scheffler went on to eagle the 13th hole on that round. He eventually won the 2024 Masters Tournament. Remember that the next time you find yourself in a day that feels like it is spiraling toward disaster. Close the door on the compartment that was the last miserable hole and saunter to the next patient like it never happened.
And maybe close the clubface a bit on address for your next drive.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on X. Write to him at dermnews@mdedge.com.
You know what the happiest animal in the world is? A goldfish. You know why? It’s got a 10-second memory. Be a goldfish. — Ted Lasso
I don’t play much golf. When I do, it’s when my dad is in town. He shoots his age (78). I shoot double mine (52). He was recently here. We played and watched the Masters where he pointed out how I looked a lot like Scottie Scheffler, the now two-time Masters champion. On the 10th hole of his third round, you could see the resemblance. Scheffler’s third shot flew past the hole into the galley. He rifled the fourth past the hole on its way back toward the fairway. It was now a good distance further from the cup than a minute ago. He proceeded to misread his bogey putt, ending his misery with a double bogey. Scheffler went on to bogey the next hole and dropped from first on the leaderboard to fifth. Yes, I looked just like that on my last round. But here is where Scheffler and I differ. After a hole like that, I’d have been apoplectic, seething with self loathing. Scheffler was not. He kept moving. Head up, he sauntered to the next hole as if he had no awareness of what just transpired.
The ability to compartmentalize is useful not only to become the Masters champion, but also to become master of your day. In this way, golf is a nice approximation for life. The best golfers in the world will always have horrible shots and dreadful holes. The winning ones are often those who recover rather than continue in a downward spiral of one bad shot after another.
It’s easy to think of regular days that went just like Scheffler’s atrocious 10th hole. Getting pimped in front of distinguished faculty at Grand Rounds and whiffing (it was Sweet Syndrome). Calling a patient to let him know that his syphilis test did in fact come back positive (it was his father on the phone, also Mr. Rodham). Arguing with a patient that a biopsy was not needed for me to diagnose her with zoster (you’ve lost once, you’ve lost your temper). Each of these made me feel like slamming my club down, quitting the round right then and there. Losing control though, leads to flubbing the next question or arguing with the following patient. The masters let it go. Like goldfish, they live in the present without any thought of what happened 10 seconds ago.
We don’t have to take advice just from Ted Lasso here; there is plenty of research to support this concept of the critical relationship between resilience and psychological flexibility. Specifically, flexible cognitive control allows us to guide attention and to choose appropriate appraisal and good coping strategies. Ultimately, this leads to better performance. You might be a skilled athlete or presenter, but if you can’t regulate your emotions and something goes wrong, then you’ll perform as poorly as an amateur.
Scheffler went on to eagle the 13th hole on that round. He eventually won the 2024 Masters Tournament. Remember that the next time you find yourself in a day that feels like it is spiraling toward disaster. Close the door on the compartment that was the last miserable hole and saunter to the next patient like it never happened.
And maybe close the clubface a bit on address for your next drive.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on X. Write to him at dermnews@mdedge.com.
Weighing the Benefits of Integrating AI-based Clinical Notes Into Your Practice
Picture a healthcare system where physicians aren’t bogged down by excessive charting but are instead fully present with their patients, offering undivided attention and personalized care. In a recent X post, Stuart Blitz, COO and co-founder of Hone Health, sparked a thought-provoking conversation. “The problem with US healthcare is physicians are burned out since they spend way too much time charting, not enough with patients,” he wrote. “If you created a health system that did zero charting, you’d attract the best physicians and all patients would go there. Who is working on this?”
This resonates with many in the medical community, myself included, because the strain of extensive documentation detracts from patient care. Having worked in both large and small healthcare systems, I know the burden of extensive charting is a palpable challenge, often detracting from the time we can devote to our patients.
The first part of this two-part series examines the overarching benefits of artificial intelligence (AI)–based clinical documentation in modern healthcare, a field witnessing a paradigm shift thanks to advancements in AI.
Transformative Evolution of Clinical Documentation
The transition from manual documentation to AI-driven solutions marks a significant shift in the field, with a number of products in development including Nuance, Abridge, Ambience, ScribeAmerica, 3M, and DeepScribe. These tools use ambient clinical intelligence (ACI) to automate documentation, capturing patient conversations and translating them into structured clinical summaries. This innovation aligns with the vision of reducing charting burdens and enhancing patient-physician interactions.
How does it work? ACI refers to a sophisticated form of AI applied in healthcare settings, particularly focusing on enhancing the clinical documentation process without disrupting the natural flow of the consultation. Here’s a technical yet practical breakdown of ACI and the algorithms it typically employs:
Data capture and processing: ACI systems employ various sensors and processing units, typically integrated into clinical settings. These sensors, like microphones and cameras, gather diverse data such as audio from patient-doctor dialogues and visual cues. This information is then processed in real-time or near–real-time.
Natural language processing (NLP): A core component of ACI is advanced NLP algorithms. These algorithms analyze the captured audio data, transcribing spoken words into text. NLP goes beyond mere transcription; it involves understanding context, extracting relevant medical information (like symptoms, diagnoses, and treatment plans), and interpreting the nuances of human language.
Deep learning: Machine learning, particularly deep-learning techniques, are employed to improve the accuracy of ACI systems continually. These algorithms can learn from vast datasets of clinical interactions, enhancing their ability to transcribe and interpret future conversations accurately. As they learn, they become better at understanding different accents, complex medical terms, and variations in speech patterns.
Integration with electronic health records (EHRs): ACI systems are often designed to integrate seamlessly with existing EHR systems. They can automatically populate patient records with information from patient-clinician interactions, reducing manual entry and potential errors.
Customization and personalization: Many ACI systems offer customizable templates or allow clinicians to tailor documentation workflows. This flexibility ensures that the output aligns with the specific needs and preferences of healthcare providers.
Ethical and privacy considerations: ACI systems must navigate significant ethical and privacy concerns, especially related to patient consent and data security. These systems need to comply with healthcare privacy regulations such as HIPAA. They need to securely manage sensitive patient data and restrict access to authorized personnel only.
Broad-Spectrum Benefits of AI in Documentation
- Reducing clinician burnout: By automating the documentation process, AI tools like DAX Copilot alleviate a significant contributor to physician burnout, enabling clinicians to focus more on patient care.
- Enhanced patient care: With AI handling documentation, clinicians can engage more with their patients, leading to improved care quality and patient satisfaction.
- Data accuracy and quality: AI-driven documentation captures detailed patient encounters accurately, ensuring high-quality and comprehensive medical records.
- Response to the growing need for efficient healthcare: AI-based documentation is a direct response to the growing call for more efficient healthcare practices, where clinicians spend less time on paperwork and more with patients.
The shift toward AI-based clinical documentation represents a critical step in addressing the inefficiencies in healthcare systems. It’s a move towards a more patient-centered approach, where clinicians can focus more on patient care by reducing the time spent on excessive charting. Hopefully, we can integrate these solutions into our clinics at a large enough scale to make such an impact.
In the next column, we will explore in-depth insights from Kenneth Harper at Nuance on the technical implementation of these tools, with DAX as an example.
I would love to read your comments on AI in clinical trials as well as other AI-related topics. Write me at Arturo.ai.medtech@gmail.com or find me on X @DrBonillaOnc.
Dr. Loaiza-Bonilla is the co-founder and chief medical officer at Massive Bio, a company connecting patients to clinical trials using artificial intelligence. His research and professional interests focus on precision medicine, clinical trial design, digital health, entrepreneurship, and patient advocacy. Dr Loaiza-Bonilla serves as medical director of oncology research at Capital Health in New Jersey, where he maintains a connection to patient care by attending to patients 2 days a week. He has served as a consultant for Verify, PSI CRO, Bayer, AstraZeneca, Cardinal Health, BrightInsight, The Lynx Group, Fresenius, Pfizer, Ipsen, and Guardant; served as a speaker or a member of a speakers bureau for Amgen, Guardant, Eisai, Ipsen, Natera, Merck, Bristol-Myers Squibb, and AstraZeneca. He holds a 5% or greater equity interest in Massive Bio.
A version of this article appeared on Medscape.com.
Picture a healthcare system where physicians aren’t bogged down by excessive charting but are instead fully present with their patients, offering undivided attention and personalized care. In a recent X post, Stuart Blitz, COO and co-founder of Hone Health, sparked a thought-provoking conversation. “The problem with US healthcare is physicians are burned out since they spend way too much time charting, not enough with patients,” he wrote. “If you created a health system that did zero charting, you’d attract the best physicians and all patients would go there. Who is working on this?”
This resonates with many in the medical community, myself included, because the strain of extensive documentation detracts from patient care. Having worked in both large and small healthcare systems, I know the burden of extensive charting is a palpable challenge, often detracting from the time we can devote to our patients.
The first part of this two-part series examines the overarching benefits of artificial intelligence (AI)–based clinical documentation in modern healthcare, a field witnessing a paradigm shift thanks to advancements in AI.
Transformative Evolution of Clinical Documentation
The transition from manual documentation to AI-driven solutions marks a significant shift in the field, with a number of products in development including Nuance, Abridge, Ambience, ScribeAmerica, 3M, and DeepScribe. These tools use ambient clinical intelligence (ACI) to automate documentation, capturing patient conversations and translating them into structured clinical summaries. This innovation aligns with the vision of reducing charting burdens and enhancing patient-physician interactions.
How does it work? ACI refers to a sophisticated form of AI applied in healthcare settings, particularly focusing on enhancing the clinical documentation process without disrupting the natural flow of the consultation. Here’s a technical yet practical breakdown of ACI and the algorithms it typically employs:
Data capture and processing: ACI systems employ various sensors and processing units, typically integrated into clinical settings. These sensors, like microphones and cameras, gather diverse data such as audio from patient-doctor dialogues and visual cues. This information is then processed in real-time or near–real-time.
Natural language processing (NLP): A core component of ACI is advanced NLP algorithms. These algorithms analyze the captured audio data, transcribing spoken words into text. NLP goes beyond mere transcription; it involves understanding context, extracting relevant medical information (like symptoms, diagnoses, and treatment plans), and interpreting the nuances of human language.
Deep learning: Machine learning, particularly deep-learning techniques, are employed to improve the accuracy of ACI systems continually. These algorithms can learn from vast datasets of clinical interactions, enhancing their ability to transcribe and interpret future conversations accurately. As they learn, they become better at understanding different accents, complex medical terms, and variations in speech patterns.
Integration with electronic health records (EHRs): ACI systems are often designed to integrate seamlessly with existing EHR systems. They can automatically populate patient records with information from patient-clinician interactions, reducing manual entry and potential errors.
Customization and personalization: Many ACI systems offer customizable templates or allow clinicians to tailor documentation workflows. This flexibility ensures that the output aligns with the specific needs and preferences of healthcare providers.
Ethical and privacy considerations: ACI systems must navigate significant ethical and privacy concerns, especially related to patient consent and data security. These systems need to comply with healthcare privacy regulations such as HIPAA. They need to securely manage sensitive patient data and restrict access to authorized personnel only.
Broad-Spectrum Benefits of AI in Documentation
- Reducing clinician burnout: By automating the documentation process, AI tools like DAX Copilot alleviate a significant contributor to physician burnout, enabling clinicians to focus more on patient care.
- Enhanced patient care: With AI handling documentation, clinicians can engage more with their patients, leading to improved care quality and patient satisfaction.
- Data accuracy and quality: AI-driven documentation captures detailed patient encounters accurately, ensuring high-quality and comprehensive medical records.
- Response to the growing need for efficient healthcare: AI-based documentation is a direct response to the growing call for more efficient healthcare practices, where clinicians spend less time on paperwork and more with patients.
The shift toward AI-based clinical documentation represents a critical step in addressing the inefficiencies in healthcare systems. It’s a move towards a more patient-centered approach, where clinicians can focus more on patient care by reducing the time spent on excessive charting. Hopefully, we can integrate these solutions into our clinics at a large enough scale to make such an impact.
In the next column, we will explore in-depth insights from Kenneth Harper at Nuance on the technical implementation of these tools, with DAX as an example.
I would love to read your comments on AI in clinical trials as well as other AI-related topics. Write me at Arturo.ai.medtech@gmail.com or find me on X @DrBonillaOnc.
Dr. Loaiza-Bonilla is the co-founder and chief medical officer at Massive Bio, a company connecting patients to clinical trials using artificial intelligence. His research and professional interests focus on precision medicine, clinical trial design, digital health, entrepreneurship, and patient advocacy. Dr Loaiza-Bonilla serves as medical director of oncology research at Capital Health in New Jersey, where he maintains a connection to patient care by attending to patients 2 days a week. He has served as a consultant for Verify, PSI CRO, Bayer, AstraZeneca, Cardinal Health, BrightInsight, The Lynx Group, Fresenius, Pfizer, Ipsen, and Guardant; served as a speaker or a member of a speakers bureau for Amgen, Guardant, Eisai, Ipsen, Natera, Merck, Bristol-Myers Squibb, and AstraZeneca. He holds a 5% or greater equity interest in Massive Bio.
A version of this article appeared on Medscape.com.
Picture a healthcare system where physicians aren’t bogged down by excessive charting but are instead fully present with their patients, offering undivided attention and personalized care. In a recent X post, Stuart Blitz, COO and co-founder of Hone Health, sparked a thought-provoking conversation. “The problem with US healthcare is physicians are burned out since they spend way too much time charting, not enough with patients,” he wrote. “If you created a health system that did zero charting, you’d attract the best physicians and all patients would go there. Who is working on this?”
This resonates with many in the medical community, myself included, because the strain of extensive documentation detracts from patient care. Having worked in both large and small healthcare systems, I know the burden of extensive charting is a palpable challenge, often detracting from the time we can devote to our patients.
The first part of this two-part series examines the overarching benefits of artificial intelligence (AI)–based clinical documentation in modern healthcare, a field witnessing a paradigm shift thanks to advancements in AI.
Transformative Evolution of Clinical Documentation
The transition from manual documentation to AI-driven solutions marks a significant shift in the field, with a number of products in development including Nuance, Abridge, Ambience, ScribeAmerica, 3M, and DeepScribe. These tools use ambient clinical intelligence (ACI) to automate documentation, capturing patient conversations and translating them into structured clinical summaries. This innovation aligns with the vision of reducing charting burdens and enhancing patient-physician interactions.
How does it work? ACI refers to a sophisticated form of AI applied in healthcare settings, particularly focusing on enhancing the clinical documentation process without disrupting the natural flow of the consultation. Here’s a technical yet practical breakdown of ACI and the algorithms it typically employs:
Data capture and processing: ACI systems employ various sensors and processing units, typically integrated into clinical settings. These sensors, like microphones and cameras, gather diverse data such as audio from patient-doctor dialogues and visual cues. This information is then processed in real-time or near–real-time.
Natural language processing (NLP): A core component of ACI is advanced NLP algorithms. These algorithms analyze the captured audio data, transcribing spoken words into text. NLP goes beyond mere transcription; it involves understanding context, extracting relevant medical information (like symptoms, diagnoses, and treatment plans), and interpreting the nuances of human language.
Deep learning: Machine learning, particularly deep-learning techniques, are employed to improve the accuracy of ACI systems continually. These algorithms can learn from vast datasets of clinical interactions, enhancing their ability to transcribe and interpret future conversations accurately. As they learn, they become better at understanding different accents, complex medical terms, and variations in speech patterns.
Integration with electronic health records (EHRs): ACI systems are often designed to integrate seamlessly with existing EHR systems. They can automatically populate patient records with information from patient-clinician interactions, reducing manual entry and potential errors.
Customization and personalization: Many ACI systems offer customizable templates or allow clinicians to tailor documentation workflows. This flexibility ensures that the output aligns with the specific needs and preferences of healthcare providers.
Ethical and privacy considerations: ACI systems must navigate significant ethical and privacy concerns, especially related to patient consent and data security. These systems need to comply with healthcare privacy regulations such as HIPAA. They need to securely manage sensitive patient data and restrict access to authorized personnel only.
Broad-Spectrum Benefits of AI in Documentation
- Reducing clinician burnout: By automating the documentation process, AI tools like DAX Copilot alleviate a significant contributor to physician burnout, enabling clinicians to focus more on patient care.
- Enhanced patient care: With AI handling documentation, clinicians can engage more with their patients, leading to improved care quality and patient satisfaction.
- Data accuracy and quality: AI-driven documentation captures detailed patient encounters accurately, ensuring high-quality and comprehensive medical records.
- Response to the growing need for efficient healthcare: AI-based documentation is a direct response to the growing call for more efficient healthcare practices, where clinicians spend less time on paperwork and more with patients.
The shift toward AI-based clinical documentation represents a critical step in addressing the inefficiencies in healthcare systems. It’s a move towards a more patient-centered approach, where clinicians can focus more on patient care by reducing the time spent on excessive charting. Hopefully, we can integrate these solutions into our clinics at a large enough scale to make such an impact.
In the next column, we will explore in-depth insights from Kenneth Harper at Nuance on the technical implementation of these tools, with DAX as an example.
I would love to read your comments on AI in clinical trials as well as other AI-related topics. Write me at Arturo.ai.medtech@gmail.com or find me on X @DrBonillaOnc.
Dr. Loaiza-Bonilla is the co-founder and chief medical officer at Massive Bio, a company connecting patients to clinical trials using artificial intelligence. His research and professional interests focus on precision medicine, clinical trial design, digital health, entrepreneurship, and patient advocacy. Dr Loaiza-Bonilla serves as medical director of oncology research at Capital Health in New Jersey, where he maintains a connection to patient care by attending to patients 2 days a week. He has served as a consultant for Verify, PSI CRO, Bayer, AstraZeneca, Cardinal Health, BrightInsight, The Lynx Group, Fresenius, Pfizer, Ipsen, and Guardant; served as a speaker or a member of a speakers bureau for Amgen, Guardant, Eisai, Ipsen, Natera, Merck, Bristol-Myers Squibb, and AstraZeneca. He holds a 5% or greater equity interest in Massive Bio.
A version of this article appeared on Medscape.com.
New Federal Rule Delivers Workplace Support, Time Off for Pregnant Docs
Pregnant physicians may receive more workplace accommodations and protection against discrimination thanks to an updated rule from the US Equal Employment Opportunity Commission (EEOC). The guidelines could prevent women from losing critical career momentum.
The Pregnant Workers Fairness Act (PWFA) aims to help workers balance professional demands with healthy pregnancies. It requires employers to provide reasonable accommodations for a “worker’s known limitations,” including physical or mental conditions associated with “pregnancy, childbirth, or related medical conditions.”
Reasonable accommodations vary but may involve time off to attend healthcare appointments or recover from childbirth, extra breaks during a shift, shorter work hours, or the ability to sit instead of stand. Private and public sector employers, including state and local governments, federal agencies, and employment agencies, must abide by the new guidelines unless they can provide evidence that doing so will cause undue hardship.
Female doctors have historically encountered significant barriers to family planning. Years of training cause them to delay having children, often leading to higher rates of infertility, miscarriage, and pregnancy complications than in the general population.
Some specialties, like surgeons, are particularly at risk, with 42% reporting at least one pregnancy loss. Most surgeons work their regular schedules until delivery despite desiring workload reductions, commonly citing unsupportive workplaces as a reason for not seeking accommodations.
Trauma surgeon Qaali Hussein, MD, became pregnant with her first child during her intern year in 2008. She told this news organization that her residency program didn’t even have a maternity policy at the time, and her male supervisor was certain that motherhood would end her surgical career.
She shared how “women usually waited until the end of their training to get pregnant. No one had ever gotten pregnant during the program and returned from maternity leave. I was the first to do so, so there wasn’t a policy or any program support to say, ‘What can we do to help?’ ”
Dr. Hussein used her vacation and sick time, returning to work 4 weeks after delivery. She had five more children, including twins her chief year and another baby during fellowship training in 2014.
Each subsequent pregnancy was met with the same response from program leadership, she recalled. “They’d say, ‘This is it. You may have been able to do the first and second child, but this one will be impossible.’ ”
After the PWFA regulations first became enforceable in June, the EEOC accepted public feedback. The guidelines received nearly 100,000 comments, spurred mainly by the inclusion of abortion care as a qualifying condition for which an employee could receive accommodations. About 54,000 comments called for abortion to be excluded from the final rule, and 40,000 supported keeping the clause.
The EEOC issued the final rule on April 15. It includes abortion care. However, the updated rule “does not require any employee to have — or not to have — an abortion, does not require taxpayers to pay for any abortions, and does not compel health care providers to provide any abortions,” the unpublished version of the final rule said. It is scheduled to take effect 60 days after its publication in the Federal Register on April 19.
Increasing Support for Doctor-Moms
The PWFA supplements other EEOC protections, such as pregnancy discrimination under Title VII of the Civil Rights Act of 1964 and access to reasonable accommodations under the Americans with Disabilities Act. In addition, it builds upon Department of Labor regulations, like the PUMP Act for breastfeeding employees and the Family and Medical Leave Act, which provides 12 weeks of unpaid, job-protected leave for the arrival of a child or certain medical conditions.
FMLA applies only to employees who have worked full-time for at least 12 months for an employer with 50 or more employees. Meanwhile, the unpaid, job-protected leave under the PWFA has no waiting period, lowers the required number of employees to 15, and permits accommodations for up to 40 weeks.
Employers are encouraged to honor “common and simple” requests, like using a closer parking space or pumping or nursing at work, without requiring a doctor’s note, the rule said.
Efforts to improve family leave policies for physicians and residents have been gaining traction. In 2021, the American Board of Medical Specialties began requiring its member boards with training programs lasting 2 or more years to allow at least 6 weeks off for parental, caregiver, and medical leave. This time can be taken without exhausting vacation or sick leave or requiring an extension in training. Over half of the 24 member boards permit leave beyond 6 weeks, including the American Boards of Allergy and Immunology, Emergency Medicine, Family Medicine, Radiology, and Surgery.
Estefania Oliveros, MD, MSc, cardiologist and assistant professor at the Lewis Katz School of Medicine at Temple University, Philadelphia, told this news organization that the Accreditation Council for Graduate Medical Education also requires that residents and fellows receive 6 weeks of paid leave.
“We add to that vacation time, so it gives them at least 8 weeks,” she said. The school has created spaces for nursing mothers — something neither she nor Dr. Hussein had access to when breastfeeding — and encourages the attendings to be proactive in excusing pregnant fellows for appointments.
This differs significantly from her fellowship training experience 6 years ago at another institution, where she worked without accommodations until the day before her cesarean delivery. Dr. Oliveros had to use all her vacation time for recovery, returning to the program after 4 weeks instead of the recommended 6.
“And that’s the story you hear all the time. Not because people are ill-intended; I just don’t think the system is designed to accommodate women, so we lose a lot of talent that way,” said Dr. Oliveros, whose 2019 survey in the Journal of the American College of Cardiology called for more support and protections for pregnant doctors.
Both doctors believe the PWFA will be beneficial but only if leadership in the field takes up the cause.
“The cultures of these institutions determine whether women feel safe or even confident enough to have children in medical school or residency,” said Dr. Hussein.
A version of this article appeared on Medscape.com.
Pregnant physicians may receive more workplace accommodations and protection against discrimination thanks to an updated rule from the US Equal Employment Opportunity Commission (EEOC). The guidelines could prevent women from losing critical career momentum.
The Pregnant Workers Fairness Act (PWFA) aims to help workers balance professional demands with healthy pregnancies. It requires employers to provide reasonable accommodations for a “worker’s known limitations,” including physical or mental conditions associated with “pregnancy, childbirth, or related medical conditions.”
Reasonable accommodations vary but may involve time off to attend healthcare appointments or recover from childbirth, extra breaks during a shift, shorter work hours, or the ability to sit instead of stand. Private and public sector employers, including state and local governments, federal agencies, and employment agencies, must abide by the new guidelines unless they can provide evidence that doing so will cause undue hardship.
Female doctors have historically encountered significant barriers to family planning. Years of training cause them to delay having children, often leading to higher rates of infertility, miscarriage, and pregnancy complications than in the general population.
Some specialties, like surgeons, are particularly at risk, with 42% reporting at least one pregnancy loss. Most surgeons work their regular schedules until delivery despite desiring workload reductions, commonly citing unsupportive workplaces as a reason for not seeking accommodations.
Trauma surgeon Qaali Hussein, MD, became pregnant with her first child during her intern year in 2008. She told this news organization that her residency program didn’t even have a maternity policy at the time, and her male supervisor was certain that motherhood would end her surgical career.
She shared how “women usually waited until the end of their training to get pregnant. No one had ever gotten pregnant during the program and returned from maternity leave. I was the first to do so, so there wasn’t a policy or any program support to say, ‘What can we do to help?’ ”
Dr. Hussein used her vacation and sick time, returning to work 4 weeks after delivery. She had five more children, including twins her chief year and another baby during fellowship training in 2014.
Each subsequent pregnancy was met with the same response from program leadership, she recalled. “They’d say, ‘This is it. You may have been able to do the first and second child, but this one will be impossible.’ ”
After the PWFA regulations first became enforceable in June, the EEOC accepted public feedback. The guidelines received nearly 100,000 comments, spurred mainly by the inclusion of abortion care as a qualifying condition for which an employee could receive accommodations. About 54,000 comments called for abortion to be excluded from the final rule, and 40,000 supported keeping the clause.
The EEOC issued the final rule on April 15. It includes abortion care. However, the updated rule “does not require any employee to have — or not to have — an abortion, does not require taxpayers to pay for any abortions, and does not compel health care providers to provide any abortions,” the unpublished version of the final rule said. It is scheduled to take effect 60 days after its publication in the Federal Register on April 19.
Increasing Support for Doctor-Moms
The PWFA supplements other EEOC protections, such as pregnancy discrimination under Title VII of the Civil Rights Act of 1964 and access to reasonable accommodations under the Americans with Disabilities Act. In addition, it builds upon Department of Labor regulations, like the PUMP Act for breastfeeding employees and the Family and Medical Leave Act, which provides 12 weeks of unpaid, job-protected leave for the arrival of a child or certain medical conditions.
FMLA applies only to employees who have worked full-time for at least 12 months for an employer with 50 or more employees. Meanwhile, the unpaid, job-protected leave under the PWFA has no waiting period, lowers the required number of employees to 15, and permits accommodations for up to 40 weeks.
Employers are encouraged to honor “common and simple” requests, like using a closer parking space or pumping or nursing at work, without requiring a doctor’s note, the rule said.
Efforts to improve family leave policies for physicians and residents have been gaining traction. In 2021, the American Board of Medical Specialties began requiring its member boards with training programs lasting 2 or more years to allow at least 6 weeks off for parental, caregiver, and medical leave. This time can be taken without exhausting vacation or sick leave or requiring an extension in training. Over half of the 24 member boards permit leave beyond 6 weeks, including the American Boards of Allergy and Immunology, Emergency Medicine, Family Medicine, Radiology, and Surgery.
Estefania Oliveros, MD, MSc, cardiologist and assistant professor at the Lewis Katz School of Medicine at Temple University, Philadelphia, told this news organization that the Accreditation Council for Graduate Medical Education also requires that residents and fellows receive 6 weeks of paid leave.
“We add to that vacation time, so it gives them at least 8 weeks,” she said. The school has created spaces for nursing mothers — something neither she nor Dr. Hussein had access to when breastfeeding — and encourages the attendings to be proactive in excusing pregnant fellows for appointments.
This differs significantly from her fellowship training experience 6 years ago at another institution, where she worked without accommodations until the day before her cesarean delivery. Dr. Oliveros had to use all her vacation time for recovery, returning to the program after 4 weeks instead of the recommended 6.
“And that’s the story you hear all the time. Not because people are ill-intended; I just don’t think the system is designed to accommodate women, so we lose a lot of talent that way,” said Dr. Oliveros, whose 2019 survey in the Journal of the American College of Cardiology called for more support and protections for pregnant doctors.
Both doctors believe the PWFA will be beneficial but only if leadership in the field takes up the cause.
“The cultures of these institutions determine whether women feel safe or even confident enough to have children in medical school or residency,” said Dr. Hussein.
A version of this article appeared on Medscape.com.
Pregnant physicians may receive more workplace accommodations and protection against discrimination thanks to an updated rule from the US Equal Employment Opportunity Commission (EEOC). The guidelines could prevent women from losing critical career momentum.
The Pregnant Workers Fairness Act (PWFA) aims to help workers balance professional demands with healthy pregnancies. It requires employers to provide reasonable accommodations for a “worker’s known limitations,” including physical or mental conditions associated with “pregnancy, childbirth, or related medical conditions.”
Reasonable accommodations vary but may involve time off to attend healthcare appointments or recover from childbirth, extra breaks during a shift, shorter work hours, or the ability to sit instead of stand. Private and public sector employers, including state and local governments, federal agencies, and employment agencies, must abide by the new guidelines unless they can provide evidence that doing so will cause undue hardship.
Female doctors have historically encountered significant barriers to family planning. Years of training cause them to delay having children, often leading to higher rates of infertility, miscarriage, and pregnancy complications than in the general population.
Some specialties, like surgeons, are particularly at risk, with 42% reporting at least one pregnancy loss. Most surgeons work their regular schedules until delivery despite desiring workload reductions, commonly citing unsupportive workplaces as a reason for not seeking accommodations.
Trauma surgeon Qaali Hussein, MD, became pregnant with her first child during her intern year in 2008. She told this news organization that her residency program didn’t even have a maternity policy at the time, and her male supervisor was certain that motherhood would end her surgical career.
She shared how “women usually waited until the end of their training to get pregnant. No one had ever gotten pregnant during the program and returned from maternity leave. I was the first to do so, so there wasn’t a policy or any program support to say, ‘What can we do to help?’ ”
Dr. Hussein used her vacation and sick time, returning to work 4 weeks after delivery. She had five more children, including twins her chief year and another baby during fellowship training in 2014.
Each subsequent pregnancy was met with the same response from program leadership, she recalled. “They’d say, ‘This is it. You may have been able to do the first and second child, but this one will be impossible.’ ”
After the PWFA regulations first became enforceable in June, the EEOC accepted public feedback. The guidelines received nearly 100,000 comments, spurred mainly by the inclusion of abortion care as a qualifying condition for which an employee could receive accommodations. About 54,000 comments called for abortion to be excluded from the final rule, and 40,000 supported keeping the clause.
The EEOC issued the final rule on April 15. It includes abortion care. However, the updated rule “does not require any employee to have — or not to have — an abortion, does not require taxpayers to pay for any abortions, and does not compel health care providers to provide any abortions,” the unpublished version of the final rule said. It is scheduled to take effect 60 days after its publication in the Federal Register on April 19.
Increasing Support for Doctor-Moms
The PWFA supplements other EEOC protections, such as pregnancy discrimination under Title VII of the Civil Rights Act of 1964 and access to reasonable accommodations under the Americans with Disabilities Act. In addition, it builds upon Department of Labor regulations, like the PUMP Act for breastfeeding employees and the Family and Medical Leave Act, which provides 12 weeks of unpaid, job-protected leave for the arrival of a child or certain medical conditions.
FMLA applies only to employees who have worked full-time for at least 12 months for an employer with 50 or more employees. Meanwhile, the unpaid, job-protected leave under the PWFA has no waiting period, lowers the required number of employees to 15, and permits accommodations for up to 40 weeks.
Employers are encouraged to honor “common and simple” requests, like using a closer parking space or pumping or nursing at work, without requiring a doctor’s note, the rule said.
Efforts to improve family leave policies for physicians and residents have been gaining traction. In 2021, the American Board of Medical Specialties began requiring its member boards with training programs lasting 2 or more years to allow at least 6 weeks off for parental, caregiver, and medical leave. This time can be taken without exhausting vacation or sick leave or requiring an extension in training. Over half of the 24 member boards permit leave beyond 6 weeks, including the American Boards of Allergy and Immunology, Emergency Medicine, Family Medicine, Radiology, and Surgery.
Estefania Oliveros, MD, MSc, cardiologist and assistant professor at the Lewis Katz School of Medicine at Temple University, Philadelphia, told this news organization that the Accreditation Council for Graduate Medical Education also requires that residents and fellows receive 6 weeks of paid leave.
“We add to that vacation time, so it gives them at least 8 weeks,” she said. The school has created spaces for nursing mothers — something neither she nor Dr. Hussein had access to when breastfeeding — and encourages the attendings to be proactive in excusing pregnant fellows for appointments.
This differs significantly from her fellowship training experience 6 years ago at another institution, where she worked without accommodations until the day before her cesarean delivery. Dr. Oliveros had to use all her vacation time for recovery, returning to the program after 4 weeks instead of the recommended 6.
“And that’s the story you hear all the time. Not because people are ill-intended; I just don’t think the system is designed to accommodate women, so we lose a lot of talent that way,” said Dr. Oliveros, whose 2019 survey in the Journal of the American College of Cardiology called for more support and protections for pregnant doctors.
Both doctors believe the PWFA will be beneficial but only if leadership in the field takes up the cause.
“The cultures of these institutions determine whether women feel safe or even confident enough to have children in medical school or residency,” said Dr. Hussein.
A version of this article appeared on Medscape.com.
AI Surpasses Harvard Docs on Clinical Reasoning Test
TOPLINE:
The AI had more instances of incorrect reasoning than the doctors did but scored better overall.
METHODOLOGY:
- The study involved 39 physicians from two academic medical centers in Boston and the generative AI model GPT-4.
- Participants were presented with 20 simulated clinical cases involving common problems such as pharyngitis, headache, abdominal pain, cough, and chest pain. Each case included sections describing the triage presentation, review of systems, physical examination, and diagnostic testing.
- The primary outcome was the Revised-IDEA (R-IDEA) score, a 10-point scale evaluating clinical reasoning documentation across four domains: Interpretive summary, differential diagnosis, explanation of the lead diagnosis, and alternative diagnoses.
TAKEAWAY:
- AI achieved a median R-IDEA score of 10, higher than attending physicians (median score, 9) and residents (8).
- The chatbot had a significantly higher estimated probability of achieving a high R-IDEA score of 8-10 (0.99) compared with attendings (0.76) and residents (0.56).
- AI provided more responses that contained instances of incorrect clinical reasoning (13.8%) than residents (2.8%) and attending physicians (12.5%). It performed similarly to physicians in diagnostic accuracy and inclusion of cannot-miss diagnoses.
IN PRACTICE:
“Future research should assess clinical reasoning of the LLM-physician interaction, as LLMs will more likely augment, not replace, the human reasoning process,” the authors of the study wrote.
SOURCE:
Adam Rodman, MD, MPH, with Beth Israel Deaconess Medical Center, Boston, was the corresponding author on the paper. The research was published online in JAMA Internal Medicine.
LIMITATIONS:
Simulated clinical cases may not replicate performance in real-world scenarios. Further training could enhance the performance of the AI, so the study may underestimate its capabilities, the researchers noted.
DISCLOSURES:
The study was supported by the Harvard Clinical and Translational Science Center and Harvard University. Authors disclosed financial ties to publishing companies and Solera Health. Dr. Rodman received funding from the Gordon and Betty Moore Foundation.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
The AI had more instances of incorrect reasoning than the doctors did but scored better overall.
METHODOLOGY:
- The study involved 39 physicians from two academic medical centers in Boston and the generative AI model GPT-4.
- Participants were presented with 20 simulated clinical cases involving common problems such as pharyngitis, headache, abdominal pain, cough, and chest pain. Each case included sections describing the triage presentation, review of systems, physical examination, and diagnostic testing.
- The primary outcome was the Revised-IDEA (R-IDEA) score, a 10-point scale evaluating clinical reasoning documentation across four domains: Interpretive summary, differential diagnosis, explanation of the lead diagnosis, and alternative diagnoses.
TAKEAWAY:
- AI achieved a median R-IDEA score of 10, higher than attending physicians (median score, 9) and residents (8).
- The chatbot had a significantly higher estimated probability of achieving a high R-IDEA score of 8-10 (0.99) compared with attendings (0.76) and residents (0.56).
- AI provided more responses that contained instances of incorrect clinical reasoning (13.8%) than residents (2.8%) and attending physicians (12.5%). It performed similarly to physicians in diagnostic accuracy and inclusion of cannot-miss diagnoses.
IN PRACTICE:
“Future research should assess clinical reasoning of the LLM-physician interaction, as LLMs will more likely augment, not replace, the human reasoning process,” the authors of the study wrote.
SOURCE:
Adam Rodman, MD, MPH, with Beth Israel Deaconess Medical Center, Boston, was the corresponding author on the paper. The research was published online in JAMA Internal Medicine.
LIMITATIONS:
Simulated clinical cases may not replicate performance in real-world scenarios. Further training could enhance the performance of the AI, so the study may underestimate its capabilities, the researchers noted.
DISCLOSURES:
The study was supported by the Harvard Clinical and Translational Science Center and Harvard University. Authors disclosed financial ties to publishing companies and Solera Health. Dr. Rodman received funding from the Gordon and Betty Moore Foundation.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
The AI had more instances of incorrect reasoning than the doctors did but scored better overall.
METHODOLOGY:
- The study involved 39 physicians from two academic medical centers in Boston and the generative AI model GPT-4.
- Participants were presented with 20 simulated clinical cases involving common problems such as pharyngitis, headache, abdominal pain, cough, and chest pain. Each case included sections describing the triage presentation, review of systems, physical examination, and diagnostic testing.
- The primary outcome was the Revised-IDEA (R-IDEA) score, a 10-point scale evaluating clinical reasoning documentation across four domains: Interpretive summary, differential diagnosis, explanation of the lead diagnosis, and alternative diagnoses.
TAKEAWAY:
- AI achieved a median R-IDEA score of 10, higher than attending physicians (median score, 9) and residents (8).
- The chatbot had a significantly higher estimated probability of achieving a high R-IDEA score of 8-10 (0.99) compared with attendings (0.76) and residents (0.56).
- AI provided more responses that contained instances of incorrect clinical reasoning (13.8%) than residents (2.8%) and attending physicians (12.5%). It performed similarly to physicians in diagnostic accuracy and inclusion of cannot-miss diagnoses.
IN PRACTICE:
“Future research should assess clinical reasoning of the LLM-physician interaction, as LLMs will more likely augment, not replace, the human reasoning process,” the authors of the study wrote.
SOURCE:
Adam Rodman, MD, MPH, with Beth Israel Deaconess Medical Center, Boston, was the corresponding author on the paper. The research was published online in JAMA Internal Medicine.
LIMITATIONS:
Simulated clinical cases may not replicate performance in real-world scenarios. Further training could enhance the performance of the AI, so the study may underestimate its capabilities, the researchers noted.
DISCLOSURES:
The study was supported by the Harvard Clinical and Translational Science Center and Harvard University. Authors disclosed financial ties to publishing companies and Solera Health. Dr. Rodman received funding from the Gordon and Betty Moore Foundation.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Childhood Loneliness Predictive of Subsequent Psychosis?
BUDAPEST, HUNGARY — Self-perceived loneliness during childhood is linked to a more than twofold increased risk for subsequent first-episode psychosis (FEP) — new findings that may point to a novel marker for the disorder.
The association between loneliness and FEP “appears to extend beyond the effects of objective social isolation,” said study presenter Covadonga M. Díaz-Caneja, MD, PhD, Institute of Psychiatry and Mental Health, Hospital General Universitario Gregorio Marañón, Madrid, and “is particularly pronounced in females.”
“These findings suggest the potential of childhood loneliness as an early risk marker for psychosis that could help guide targeted interventions,” she added.
The results were presented at the European Psychiatric Association 2024 Congress.
Isolation a Major Risk Factor
There are two components to isolation, both of which are “major risk factors” for morbidity, mortality, and the onset of mental disorders, said Dr. Díaz-Caneja.
The first is “objective social isolation,” which consists of a demonstrable lack of social connections, including social interactions, contacts, and relationships, while the other is a perceived sense of isolation, or “loneliness,” defined as a “subjective feeling of distress associated with a lack of meaningful relationships,” regardless of the amount of actual social contact an individual experiences.
Childhood loneliness occurs before age 12 and is becoming increasingly prevalent, said Dr. Díaz-Caneja. A recent survey shows that approximately one third of children report they often feel lonely.
Genetic and observational research has shown there is a bidirectional relationship between loneliness and psychosis and that patients with schizophrenia are more likely to report loneliness than is the general population.
Dr. Díaz-Caneja noted that there is no previous research that has assessed the potential association between childhood loneliness and subsequent psychosis.
To investigate, the researchers conducted an observational, case-control study in seven university hospitals in Madrid. It included individuals aged 7-40 years, including FEP patients with a psychosis duration of less than 2 years, and healthy controls from the same geographic areas.
They assessed childhood objective social isolation using the Premorbid Adjustment Scale and examined childhood loneliness with the single item: “Have you ever felt lonely for more than 6 months before the age of 12?”
A range of measures and questionnaires were also administered to assess participants’ symptom scores, alongside the Global Assessment of Functioning (GAF).
Alone vs Lonely
Two hundred eighty-five patients with FEP participated in the study. They had a mean age of 24.5 years, and 32.6% were female. The study also included 261 healthy controls (average age, 25.9 years; 48.7% female).
After the researchers adjusted for age, gender, ethnicity, and socioeconomic status, loneliness during childhood was associated with a significantly increased risk for FEP (odds ratio [OR], 2.17; 95% CI, 1.40-3.51), which increased (OR, 2.70; 95% CI, 1.58-4.62) after further adjustment for objective social isolation.
Further analysis revealed that in those who did not have objective social isolation in childhood, loneliness was associated with a significantly increased risk for FEP (OR, 2.68; 95% CI, 1.56-4.60).
However, the relationship between loneliness and FEP was not significant in participants who were objectively socially isolated during childhood (OR, 0.33; 95% CI, 0.08-1.45).
Compared with males, females reporting loneliness had a markedly increased risk for FEP (OR, 4.74; 95% CI, 2.23-10.05 vs OR, 1.17; 95% CI, 0.63-2.19).
However, females had a reduced risk of receiving a diagnosis of schizophrenia spectrum disorder (OR, 0.155; 95% CI, 0.048-0.506), indicating that loneliness influenced the type of diagnosis, she noted.
There was a significant positive relationship between loneliness in childhood and symptom scores in men, and a negative association with GAF scores in men.
Dr. Díaz-Caneja noted that the study is preliminary and a “work in progress.” The investigators plan to increase the sample size and will conduct more complex analyses, she said.
“We also of course have to bear in mind that it is a cross-sectional study and that there may be some kind of recall biases [because] we are asking patients now about what happened in the past.”
She noted that it’s unclear whether the results can be extrapolated to individuals who are currently experiencing loneliness because “the determinants of loneliness 10 years ago or 15 years ago may be different.”
How, When to Intervene
Session chair Judit Lazáry, MD, PhD, Department of Clinical and Theoretical Mental Health, Kútvölgyi Clinical Center, Semmelweis University, Budapest, Hungary, told this news organization that the association between loneliness and FEP was “not surprising.”
She explained there are a lot of data indicating that premorbid symptoms in childhood are “predictive signs for the later onset of psychosis,” and loneliness may be “a part of that.”
Individuals experiencing loneliness are more anxious and have difficulties in cultivating and maintaining relationships. In addition, they tend to socially isolate, she said.
The key question, said Dr. Lazáry, is: “How can we intervene to prevent the onset of psychosis? What is the point at which we can support the young person?”
This is challenging, she added, because while “you can detect that a kid is always alone, you cannot detect the feeling of loneliness,” and children can’t always easily express themselves.
Another potential confounder is that in adults with current psychosis, the self-perception that they were lonely during childhood may be a consequence of the disorder.
In addition, she said, individuals with psychosis often experience cognitive impairment, which could affect memory reliability.
Nevertheless, said Dr. Lazáry, the study’s findings suggest that a young person reporting loneliness in childhood may be “another symptom that we have to investigate.”
No funding was declared.
Dr. Díaz-Caneja declared a relationship with Angelini, Janssen, and Viatris and grant support from Instituto de Salud Carlos III, the Spanish Ministry of Science and Innovation, and the European Commission.
A version of this article appeared on Medscape.com.
BUDAPEST, HUNGARY — Self-perceived loneliness during childhood is linked to a more than twofold increased risk for subsequent first-episode psychosis (FEP) — new findings that may point to a novel marker for the disorder.
The association between loneliness and FEP “appears to extend beyond the effects of objective social isolation,” said study presenter Covadonga M. Díaz-Caneja, MD, PhD, Institute of Psychiatry and Mental Health, Hospital General Universitario Gregorio Marañón, Madrid, and “is particularly pronounced in females.”
“These findings suggest the potential of childhood loneliness as an early risk marker for psychosis that could help guide targeted interventions,” she added.
The results were presented at the European Psychiatric Association 2024 Congress.
Isolation a Major Risk Factor
There are two components to isolation, both of which are “major risk factors” for morbidity, mortality, and the onset of mental disorders, said Dr. Díaz-Caneja.
The first is “objective social isolation,” which consists of a demonstrable lack of social connections, including social interactions, contacts, and relationships, while the other is a perceived sense of isolation, or “loneliness,” defined as a “subjective feeling of distress associated with a lack of meaningful relationships,” regardless of the amount of actual social contact an individual experiences.
Childhood loneliness occurs before age 12 and is becoming increasingly prevalent, said Dr. Díaz-Caneja. A recent survey shows that approximately one third of children report they often feel lonely.
Genetic and observational research has shown there is a bidirectional relationship between loneliness and psychosis and that patients with schizophrenia are more likely to report loneliness than is the general population.
Dr. Díaz-Caneja noted that there is no previous research that has assessed the potential association between childhood loneliness and subsequent psychosis.
To investigate, the researchers conducted an observational, case-control study in seven university hospitals in Madrid. It included individuals aged 7-40 years, including FEP patients with a psychosis duration of less than 2 years, and healthy controls from the same geographic areas.
They assessed childhood objective social isolation using the Premorbid Adjustment Scale and examined childhood loneliness with the single item: “Have you ever felt lonely for more than 6 months before the age of 12?”
A range of measures and questionnaires were also administered to assess participants’ symptom scores, alongside the Global Assessment of Functioning (GAF).
Alone vs Lonely
Two hundred eighty-five patients with FEP participated in the study. They had a mean age of 24.5 years, and 32.6% were female. The study also included 261 healthy controls (average age, 25.9 years; 48.7% female).
After the researchers adjusted for age, gender, ethnicity, and socioeconomic status, loneliness during childhood was associated with a significantly increased risk for FEP (odds ratio [OR], 2.17; 95% CI, 1.40-3.51), which increased (OR, 2.70; 95% CI, 1.58-4.62) after further adjustment for objective social isolation.
Further analysis revealed that in those who did not have objective social isolation in childhood, loneliness was associated with a significantly increased risk for FEP (OR, 2.68; 95% CI, 1.56-4.60).
However, the relationship between loneliness and FEP was not significant in participants who were objectively socially isolated during childhood (OR, 0.33; 95% CI, 0.08-1.45).
Compared with males, females reporting loneliness had a markedly increased risk for FEP (OR, 4.74; 95% CI, 2.23-10.05 vs OR, 1.17; 95% CI, 0.63-2.19).
However, females had a reduced risk of receiving a diagnosis of schizophrenia spectrum disorder (OR, 0.155; 95% CI, 0.048-0.506), indicating that loneliness influenced the type of diagnosis, she noted.
There was a significant positive relationship between loneliness in childhood and symptom scores in men, and a negative association with GAF scores in men.
Dr. Díaz-Caneja noted that the study is preliminary and a “work in progress.” The investigators plan to increase the sample size and will conduct more complex analyses, she said.
“We also of course have to bear in mind that it is a cross-sectional study and that there may be some kind of recall biases [because] we are asking patients now about what happened in the past.”
She noted that it’s unclear whether the results can be extrapolated to individuals who are currently experiencing loneliness because “the determinants of loneliness 10 years ago or 15 years ago may be different.”
How, When to Intervene
Session chair Judit Lazáry, MD, PhD, Department of Clinical and Theoretical Mental Health, Kútvölgyi Clinical Center, Semmelweis University, Budapest, Hungary, told this news organization that the association between loneliness and FEP was “not surprising.”
She explained there are a lot of data indicating that premorbid symptoms in childhood are “predictive signs for the later onset of psychosis,” and loneliness may be “a part of that.”
Individuals experiencing loneliness are more anxious and have difficulties in cultivating and maintaining relationships. In addition, they tend to socially isolate, she said.
The key question, said Dr. Lazáry, is: “How can we intervene to prevent the onset of psychosis? What is the point at which we can support the young person?”
This is challenging, she added, because while “you can detect that a kid is always alone, you cannot detect the feeling of loneliness,” and children can’t always easily express themselves.
Another potential confounder is that in adults with current psychosis, the self-perception that they were lonely during childhood may be a consequence of the disorder.
In addition, she said, individuals with psychosis often experience cognitive impairment, which could affect memory reliability.
Nevertheless, said Dr. Lazáry, the study’s findings suggest that a young person reporting loneliness in childhood may be “another symptom that we have to investigate.”
No funding was declared.
Dr. Díaz-Caneja declared a relationship with Angelini, Janssen, and Viatris and grant support from Instituto de Salud Carlos III, the Spanish Ministry of Science and Innovation, and the European Commission.
A version of this article appeared on Medscape.com.
BUDAPEST, HUNGARY — Self-perceived loneliness during childhood is linked to a more than twofold increased risk for subsequent first-episode psychosis (FEP) — new findings that may point to a novel marker for the disorder.
The association between loneliness and FEP “appears to extend beyond the effects of objective social isolation,” said study presenter Covadonga M. Díaz-Caneja, MD, PhD, Institute of Psychiatry and Mental Health, Hospital General Universitario Gregorio Marañón, Madrid, and “is particularly pronounced in females.”
“These findings suggest the potential of childhood loneliness as an early risk marker for psychosis that could help guide targeted interventions,” she added.
The results were presented at the European Psychiatric Association 2024 Congress.
Isolation a Major Risk Factor
There are two components to isolation, both of which are “major risk factors” for morbidity, mortality, and the onset of mental disorders, said Dr. Díaz-Caneja.
The first is “objective social isolation,” which consists of a demonstrable lack of social connections, including social interactions, contacts, and relationships, while the other is a perceived sense of isolation, or “loneliness,” defined as a “subjective feeling of distress associated with a lack of meaningful relationships,” regardless of the amount of actual social contact an individual experiences.
Childhood loneliness occurs before age 12 and is becoming increasingly prevalent, said Dr. Díaz-Caneja. A recent survey shows that approximately one third of children report they often feel lonely.
Genetic and observational research has shown there is a bidirectional relationship between loneliness and psychosis and that patients with schizophrenia are more likely to report loneliness than is the general population.
Dr. Díaz-Caneja noted that there is no previous research that has assessed the potential association between childhood loneliness and subsequent psychosis.
To investigate, the researchers conducted an observational, case-control study in seven university hospitals in Madrid. It included individuals aged 7-40 years, including FEP patients with a psychosis duration of less than 2 years, and healthy controls from the same geographic areas.
They assessed childhood objective social isolation using the Premorbid Adjustment Scale and examined childhood loneliness with the single item: “Have you ever felt lonely for more than 6 months before the age of 12?”
A range of measures and questionnaires were also administered to assess participants’ symptom scores, alongside the Global Assessment of Functioning (GAF).
Alone vs Lonely
Two hundred eighty-five patients with FEP participated in the study. They had a mean age of 24.5 years, and 32.6% were female. The study also included 261 healthy controls (average age, 25.9 years; 48.7% female).
After the researchers adjusted for age, gender, ethnicity, and socioeconomic status, loneliness during childhood was associated with a significantly increased risk for FEP (odds ratio [OR], 2.17; 95% CI, 1.40-3.51), which increased (OR, 2.70; 95% CI, 1.58-4.62) after further adjustment for objective social isolation.
Further analysis revealed that in those who did not have objective social isolation in childhood, loneliness was associated with a significantly increased risk for FEP (OR, 2.68; 95% CI, 1.56-4.60).
However, the relationship between loneliness and FEP was not significant in participants who were objectively socially isolated during childhood (OR, 0.33; 95% CI, 0.08-1.45).
Compared with males, females reporting loneliness had a markedly increased risk for FEP (OR, 4.74; 95% CI, 2.23-10.05 vs OR, 1.17; 95% CI, 0.63-2.19).
However, females had a reduced risk of receiving a diagnosis of schizophrenia spectrum disorder (OR, 0.155; 95% CI, 0.048-0.506), indicating that loneliness influenced the type of diagnosis, she noted.
There was a significant positive relationship between loneliness in childhood and symptom scores in men, and a negative association with GAF scores in men.
Dr. Díaz-Caneja noted that the study is preliminary and a “work in progress.” The investigators plan to increase the sample size and will conduct more complex analyses, she said.
“We also of course have to bear in mind that it is a cross-sectional study and that there may be some kind of recall biases [because] we are asking patients now about what happened in the past.”
She noted that it’s unclear whether the results can be extrapolated to individuals who are currently experiencing loneliness because “the determinants of loneliness 10 years ago or 15 years ago may be different.”
How, When to Intervene
Session chair Judit Lazáry, MD, PhD, Department of Clinical and Theoretical Mental Health, Kútvölgyi Clinical Center, Semmelweis University, Budapest, Hungary, told this news organization that the association between loneliness and FEP was “not surprising.”
She explained there are a lot of data indicating that premorbid symptoms in childhood are “predictive signs for the later onset of psychosis,” and loneliness may be “a part of that.”
Individuals experiencing loneliness are more anxious and have difficulties in cultivating and maintaining relationships. In addition, they tend to socially isolate, she said.
The key question, said Dr. Lazáry, is: “How can we intervene to prevent the onset of psychosis? What is the point at which we can support the young person?”
This is challenging, she added, because while “you can detect that a kid is always alone, you cannot detect the feeling of loneliness,” and children can’t always easily express themselves.
Another potential confounder is that in adults with current psychosis, the self-perception that they were lonely during childhood may be a consequence of the disorder.
In addition, she said, individuals with psychosis often experience cognitive impairment, which could affect memory reliability.
Nevertheless, said Dr. Lazáry, the study’s findings suggest that a young person reporting loneliness in childhood may be “another symptom that we have to investigate.”
No funding was declared.
Dr. Díaz-Caneja declared a relationship with Angelini, Janssen, and Viatris and grant support from Instituto de Salud Carlos III, the Spanish Ministry of Science and Innovation, and the European Commission.
A version of this article appeared on Medscape.com.