User login
For MD-IQ only
New Trials in Prostate Cancer: Could Your Patient Benefit?
Metastatic castration-sensitive prostate cancer
Adults with this diagnosis may be interested in a randomized, double-blind, phase 3 study examining whether an experimental poly (ADP-ribose) polymerase (PARP) inhibitor called saruparib can further delay disease progression when added to a next-generation hormonal agent such as abiraterone (Zytiga), darolutamide (Nubeqa), or enzalutamide (Xtandi).
One group of participants will take daily oral doses of saruparib plus physician’s choice of a next-generation hormonal agent until disease progression or another reason for stopping therapy. The other group will add a placebo to a next-generation hormonal agent.
Sites in Rhode Island, Arkansas, California, Michigan, Australia, Canada, Japan, Taiwan, Thailand, the United Kingdom, and South Korea began seeking the trial’s 1800 participants in November 2023. Research centers in 31 other US states and 18 other countries are gearing up. The primary endpoint is radiographic progression-free survival. Overall survival and quality of life (QoL) are secondary endpoints. More details at clinicaltrials.gov.
This news organization asked Marc Garnick, MD, professor of medicine, Harvard Medical School and Beth Israel Deaconess Medical Center, Boston, for his take on the trial. “The study is interesting since it is adding to the evaluations of continued intensification for first-line therapy and will help further elucidate the role of PARP inhibition regardless of homologous repair status,” Dr. Garnick said. “Plus, saruparib is supposedly more selective on PARP1, which in-and-of-itself is of potential benefit.”
Metastatic castration-resistant prostate cancer
People with this type of cancer who have progressed on a next-generation hormonal agent may be eligible for a randomized, open-label, phase 3 trial testing an investigational oral treatment called MK-5684 to see if it increases survival more effectively than switching to an alternative next-generation hormonal agent.
MK-5684 is designed to inhibit the CYP11A1 enzyme, thereby disrupting the androgen-receptor signaling pathway.
One group will take twice-daily tablets of MK-5684 plus hormone replacement therapy, oral dexamethasone, and oral fludrocortisone acetate (Florinef), with rescue hydrocortisone as needed. The other participants will take daily tablets of a next-generation hormonal agent: Either enzalutamide or abiraterone. Patients assigned to abiraterone will also be given prednisone tablets.
US-based sites in nine states and Puerto Rico started looking for the trial’s 1500 participants in December 2023 in partnership with study centers in Australia, Israel, South Korea, and Taiwan. The primary endpoints are radiographic progression-free survival and overall survival. QoL will not be tracked. More details at clinicaltrials.gov.
Metastatic castration-resistant prostate cancer
Patients in this situation who have progressed on taxane-based chemotherapy as well as a next-generation hormonal agent have the option to enroll in another phase 3 MK-5684 study.
Like the trial described above, all patients will remain on their respective therapy until disease progression. In this trial, one group will take twice-daily tablets of MK-5684 without hormone replacement therapy but the same mix of oral dexamethasone and fludrocortisone. Rescue hydrocortisone will also be available. The second group will be assigned either enzalutamide or abiraterone plus prednisone.
Sites in Puerto Rico, Colorado, Nevada, and Virginia, and five other countries outside the United States, opened their doors to the first of 1200 patients in December 2023. The primary endpoints are radiographic progression-free survival and overall survival, analyzed separately for patients with and without an androgen receptor ligand-binding domain mutation. QoL will not be measured. More details at clinicaltrials.gov.
High-risk prostate cancer
People with this diagnosis can join a randomized, open-label, phase 3 National Cancer Institute study to test whether stereotactic body radiation therapy (SBRT) is as effective as conventional external beam radiation therapy (EBRT) at preventing metastasis.
SBRT delivers radiation to tumors with higher precision than EBRT. The advantage of SBRT is the ability to deliver fewer doses over a shorter duration with less collateral damage to surrounding tissues.
In the trial, half of participants will undergo five treatments of SBRT over 2 weeks, while the other half will receive 20-45 treatments of EBRT over 4-9 weeks. Study sites in 14 US states began recruiting the trial’s 1209 participants in November 2023. Metastasis-free survival over 15 years is the primary endpoint, overall survival is a secondary endpoint, and QoL measures, apart from fatigue, will not be tracked. More details at clinicaltrials.gov.
Dr. Garnick viewed this study as “problematic because patient accrual ends in 2036 with a readout in 2041.” He added, “What its relevance will be at that time is unlikely to provide practice changes, since in that interval there will undoubtedly be multiple advances in place.”
Newly diagnosed favorable intermediate risk prostate cancer
People with this type of cancer are eligible for an open-label, phase 4 real-world study of a radioactive diagnostic agent called piflufolastat F 18 (Pylarify) that targets prostate-specific membrane antigen (PSMA)–positive lesions. Piflufolastat is designed to enhance detection of metastases during PSMA-targeted PET.
Participants will receive a single injection of piflufolastat followed 1-2 hours later by a single whole-body PET-CT or PET-MRI scan. A study site at the Hoag Cancer Center in Irvine, California, welcomed the first of the trial’s 274 participants in February 2024. Sites in Tower Urology, Los Angeles, and the Cleveland Clinic, Ohio, are gearing up. Detection rate is the primary endpoint. Overall survival and QoL are not measured. More details at clinicaltrials.gov
Stages I-IV prostate cancer without bone metastases. People 60 years or older with this type of prostate cancer who are just starting androgen deprivation therapy are eligible for a phase 3, placebo-controlled trial investigating whether high-dose vitamin D can prevent or reduce androgen-deprivation therapy-induced bone loss.
For 1 year, participants will take tablets of high-dose vitamin D or a placebo and then undergo dual x-ray absorptiometry. The Ochsner Medical Center in Jefferson, Louisiana, started recruiting 366 trial participants in December 2023. Reduction in bone mineral density loss in the hip and spine over 1 year is the primary objective. QoL is a secondary objective, and overall survival will not be measured. More details at clinicaltrials.gov
Dr. Garnick expressed some concerns with the trial design so far, including that “the dose of vitamin D is not delineated nor is the target vitamin D level.”
All trial information is from the National Institutes of Health’s National Library of Medicine (online at clinicaltrials.gov). Dr. Garnick did not report conflicts with any of the trials.
A version of this article appeared on Medscape.com.
Metastatic castration-sensitive prostate cancer
Adults with this diagnosis may be interested in a randomized, double-blind, phase 3 study examining whether an experimental poly (ADP-ribose) polymerase (PARP) inhibitor called saruparib can further delay disease progression when added to a next-generation hormonal agent such as abiraterone (Zytiga), darolutamide (Nubeqa), or enzalutamide (Xtandi).
One group of participants will take daily oral doses of saruparib plus physician’s choice of a next-generation hormonal agent until disease progression or another reason for stopping therapy. The other group will add a placebo to a next-generation hormonal agent.
Sites in Rhode Island, Arkansas, California, Michigan, Australia, Canada, Japan, Taiwan, Thailand, the United Kingdom, and South Korea began seeking the trial’s 1800 participants in November 2023. Research centers in 31 other US states and 18 other countries are gearing up. The primary endpoint is radiographic progression-free survival. Overall survival and quality of life (QoL) are secondary endpoints. More details at clinicaltrials.gov.
This news organization asked Marc Garnick, MD, professor of medicine, Harvard Medical School and Beth Israel Deaconess Medical Center, Boston, for his take on the trial. “The study is interesting since it is adding to the evaluations of continued intensification for first-line therapy and will help further elucidate the role of PARP inhibition regardless of homologous repair status,” Dr. Garnick said. “Plus, saruparib is supposedly more selective on PARP1, which in-and-of-itself is of potential benefit.”
Metastatic castration-resistant prostate cancer
People with this type of cancer who have progressed on a next-generation hormonal agent may be eligible for a randomized, open-label, phase 3 trial testing an investigational oral treatment called MK-5684 to see if it increases survival more effectively than switching to an alternative next-generation hormonal agent.
MK-5684 is designed to inhibit the CYP11A1 enzyme, thereby disrupting the androgen-receptor signaling pathway.
One group will take twice-daily tablets of MK-5684 plus hormone replacement therapy, oral dexamethasone, and oral fludrocortisone acetate (Florinef), with rescue hydrocortisone as needed. The other participants will take daily tablets of a next-generation hormonal agent: Either enzalutamide or abiraterone. Patients assigned to abiraterone will also be given prednisone tablets.
US-based sites in nine states and Puerto Rico started looking for the trial’s 1500 participants in December 2023 in partnership with study centers in Australia, Israel, South Korea, and Taiwan. The primary endpoints are radiographic progression-free survival and overall survival. QoL will not be tracked. More details at clinicaltrials.gov.
Metastatic castration-resistant prostate cancer
Patients in this situation who have progressed on taxane-based chemotherapy as well as a next-generation hormonal agent have the option to enroll in another phase 3 MK-5684 study.
Like the trial described above, all patients will remain on their respective therapy until disease progression. In this trial, one group will take twice-daily tablets of MK-5684 without hormone replacement therapy but the same mix of oral dexamethasone and fludrocortisone. Rescue hydrocortisone will also be available. The second group will be assigned either enzalutamide or abiraterone plus prednisone.
Sites in Puerto Rico, Colorado, Nevada, and Virginia, and five other countries outside the United States, opened their doors to the first of 1200 patients in December 2023. The primary endpoints are radiographic progression-free survival and overall survival, analyzed separately for patients with and without an androgen receptor ligand-binding domain mutation. QoL will not be measured. More details at clinicaltrials.gov.
High-risk prostate cancer
People with this diagnosis can join a randomized, open-label, phase 3 National Cancer Institute study to test whether stereotactic body radiation therapy (SBRT) is as effective as conventional external beam radiation therapy (EBRT) at preventing metastasis.
SBRT delivers radiation to tumors with higher precision than EBRT. The advantage of SBRT is the ability to deliver fewer doses over a shorter duration with less collateral damage to surrounding tissues.
In the trial, half of participants will undergo five treatments of SBRT over 2 weeks, while the other half will receive 20-45 treatments of EBRT over 4-9 weeks. Study sites in 14 US states began recruiting the trial’s 1209 participants in November 2023. Metastasis-free survival over 15 years is the primary endpoint, overall survival is a secondary endpoint, and QoL measures, apart from fatigue, will not be tracked. More details at clinicaltrials.gov.
Dr. Garnick viewed this study as “problematic because patient accrual ends in 2036 with a readout in 2041.” He added, “What its relevance will be at that time is unlikely to provide practice changes, since in that interval there will undoubtedly be multiple advances in place.”
Newly diagnosed favorable intermediate risk prostate cancer
People with this type of cancer are eligible for an open-label, phase 4 real-world study of a radioactive diagnostic agent called piflufolastat F 18 (Pylarify) that targets prostate-specific membrane antigen (PSMA)–positive lesions. Piflufolastat is designed to enhance detection of metastases during PSMA-targeted PET.
Participants will receive a single injection of piflufolastat followed 1-2 hours later by a single whole-body PET-CT or PET-MRI scan. A study site at the Hoag Cancer Center in Irvine, California, welcomed the first of the trial’s 274 participants in February 2024. Sites in Tower Urology, Los Angeles, and the Cleveland Clinic, Ohio, are gearing up. Detection rate is the primary endpoint. Overall survival and QoL are not measured. More details at clinicaltrials.gov
Stages I-IV prostate cancer without bone metastases. People 60 years or older with this type of prostate cancer who are just starting androgen deprivation therapy are eligible for a phase 3, placebo-controlled trial investigating whether high-dose vitamin D can prevent or reduce androgen-deprivation therapy-induced bone loss.
For 1 year, participants will take tablets of high-dose vitamin D or a placebo and then undergo dual x-ray absorptiometry. The Ochsner Medical Center in Jefferson, Louisiana, started recruiting 366 trial participants in December 2023. Reduction in bone mineral density loss in the hip and spine over 1 year is the primary objective. QoL is a secondary objective, and overall survival will not be measured. More details at clinicaltrials.gov
Dr. Garnick expressed some concerns with the trial design so far, including that “the dose of vitamin D is not delineated nor is the target vitamin D level.”
All trial information is from the National Institutes of Health’s National Library of Medicine (online at clinicaltrials.gov). Dr. Garnick did not report conflicts with any of the trials.
A version of this article appeared on Medscape.com.
Metastatic castration-sensitive prostate cancer
Adults with this diagnosis may be interested in a randomized, double-blind, phase 3 study examining whether an experimental poly (ADP-ribose) polymerase (PARP) inhibitor called saruparib can further delay disease progression when added to a next-generation hormonal agent such as abiraterone (Zytiga), darolutamide (Nubeqa), or enzalutamide (Xtandi).
One group of participants will take daily oral doses of saruparib plus physician’s choice of a next-generation hormonal agent until disease progression or another reason for stopping therapy. The other group will add a placebo to a next-generation hormonal agent.
Sites in Rhode Island, Arkansas, California, Michigan, Australia, Canada, Japan, Taiwan, Thailand, the United Kingdom, and South Korea began seeking the trial’s 1800 participants in November 2023. Research centers in 31 other US states and 18 other countries are gearing up. The primary endpoint is radiographic progression-free survival. Overall survival and quality of life (QoL) are secondary endpoints. More details at clinicaltrials.gov.
This news organization asked Marc Garnick, MD, professor of medicine, Harvard Medical School and Beth Israel Deaconess Medical Center, Boston, for his take on the trial. “The study is interesting since it is adding to the evaluations of continued intensification for first-line therapy and will help further elucidate the role of PARP inhibition regardless of homologous repair status,” Dr. Garnick said. “Plus, saruparib is supposedly more selective on PARP1, which in-and-of-itself is of potential benefit.”
Metastatic castration-resistant prostate cancer
People with this type of cancer who have progressed on a next-generation hormonal agent may be eligible for a randomized, open-label, phase 3 trial testing an investigational oral treatment called MK-5684 to see if it increases survival more effectively than switching to an alternative next-generation hormonal agent.
MK-5684 is designed to inhibit the CYP11A1 enzyme, thereby disrupting the androgen-receptor signaling pathway.
One group will take twice-daily tablets of MK-5684 plus hormone replacement therapy, oral dexamethasone, and oral fludrocortisone acetate (Florinef), with rescue hydrocortisone as needed. The other participants will take daily tablets of a next-generation hormonal agent: Either enzalutamide or abiraterone. Patients assigned to abiraterone will also be given prednisone tablets.
US-based sites in nine states and Puerto Rico started looking for the trial’s 1500 participants in December 2023 in partnership with study centers in Australia, Israel, South Korea, and Taiwan. The primary endpoints are radiographic progression-free survival and overall survival. QoL will not be tracked. More details at clinicaltrials.gov.
Metastatic castration-resistant prostate cancer
Patients in this situation who have progressed on taxane-based chemotherapy as well as a next-generation hormonal agent have the option to enroll in another phase 3 MK-5684 study.
Like the trial described above, all patients will remain on their respective therapy until disease progression. In this trial, one group will take twice-daily tablets of MK-5684 without hormone replacement therapy but the same mix of oral dexamethasone and fludrocortisone. Rescue hydrocortisone will also be available. The second group will be assigned either enzalutamide or abiraterone plus prednisone.
Sites in Puerto Rico, Colorado, Nevada, and Virginia, and five other countries outside the United States, opened their doors to the first of 1200 patients in December 2023. The primary endpoints are radiographic progression-free survival and overall survival, analyzed separately for patients with and without an androgen receptor ligand-binding domain mutation. QoL will not be measured. More details at clinicaltrials.gov.
High-risk prostate cancer
People with this diagnosis can join a randomized, open-label, phase 3 National Cancer Institute study to test whether stereotactic body radiation therapy (SBRT) is as effective as conventional external beam radiation therapy (EBRT) at preventing metastasis.
SBRT delivers radiation to tumors with higher precision than EBRT. The advantage of SBRT is the ability to deliver fewer doses over a shorter duration with less collateral damage to surrounding tissues.
In the trial, half of participants will undergo five treatments of SBRT over 2 weeks, while the other half will receive 20-45 treatments of EBRT over 4-9 weeks. Study sites in 14 US states began recruiting the trial’s 1209 participants in November 2023. Metastasis-free survival over 15 years is the primary endpoint, overall survival is a secondary endpoint, and QoL measures, apart from fatigue, will not be tracked. More details at clinicaltrials.gov.
Dr. Garnick viewed this study as “problematic because patient accrual ends in 2036 with a readout in 2041.” He added, “What its relevance will be at that time is unlikely to provide practice changes, since in that interval there will undoubtedly be multiple advances in place.”
Newly diagnosed favorable intermediate risk prostate cancer
People with this type of cancer are eligible for an open-label, phase 4 real-world study of a radioactive diagnostic agent called piflufolastat F 18 (Pylarify) that targets prostate-specific membrane antigen (PSMA)–positive lesions. Piflufolastat is designed to enhance detection of metastases during PSMA-targeted PET.
Participants will receive a single injection of piflufolastat followed 1-2 hours later by a single whole-body PET-CT or PET-MRI scan. A study site at the Hoag Cancer Center in Irvine, California, welcomed the first of the trial’s 274 participants in February 2024. Sites in Tower Urology, Los Angeles, and the Cleveland Clinic, Ohio, are gearing up. Detection rate is the primary endpoint. Overall survival and QoL are not measured. More details at clinicaltrials.gov
Stages I-IV prostate cancer without bone metastases. People 60 years or older with this type of prostate cancer who are just starting androgen deprivation therapy are eligible for a phase 3, placebo-controlled trial investigating whether high-dose vitamin D can prevent or reduce androgen-deprivation therapy-induced bone loss.
For 1 year, participants will take tablets of high-dose vitamin D or a placebo and then undergo dual x-ray absorptiometry. The Ochsner Medical Center in Jefferson, Louisiana, started recruiting 366 trial participants in December 2023. Reduction in bone mineral density loss in the hip and spine over 1 year is the primary objective. QoL is a secondary objective, and overall survival will not be measured. More details at clinicaltrials.gov
Dr. Garnick expressed some concerns with the trial design so far, including that “the dose of vitamin D is not delineated nor is the target vitamin D level.”
All trial information is from the National Institutes of Health’s National Library of Medicine (online at clinicaltrials.gov). Dr. Garnick did not report conflicts with any of the trials.
A version of this article appeared on Medscape.com.
Prostate Cancer Tsunami Coming, Experts Caution
An “inevitable” global surge in prostate cancer is coming, with a worldwide doubling of cases to 2.9 million and an 85% increase in deaths to nearly 700,000 by the year 2040, the Lancet Commission on Prostate Cancer warned this week.
At a meeting of urologists in Paris, the commission said that the acceleration is already underway in high-income countries such as the United States and the United Kingdom but will gain momentum in low- and medium-income countries.
Nick James, MD, lead author of The Lancet report and professor of prostate and bladder cancer research at The Institute of Cancer Research in London, said that the surge, in part, is a medical success story.
Dr. James told this news organization.
“There is a big rise in the high-income countries. But we’re going to see a big rise in the number of 50-, 60-, 70-year-olds in the coming decades in the poorer countries, and with that comes more prostate cancer. High-income countries such as the UK and USA will also see smaller increases for the same reason.”
According to the report, to be presented April 6 at the 2024 European Association of Urology Congress in Paris, “The case for prostate cancer screening for all men aged 50-70 years (and all men of African origin aged 45–70 years) in high-income countries is strengthening with improved use of technologies such as MRI and growing evidence for the safety of active surveillance.”
Andrew Vickers, PhD, a biostatistician at Memorial Sloan Kettering Cancer Center in New York City, said that the Lancet Commission came to similar conclusions as he and an international group of researchers did in a 2023 policy paper in The BMJ. A major gap, Dr. Vickers said, is misuse of prostate-specific antigen (PSA) screening.
“We found that the ubiquitous policy compromise of letting patients decide for themselves about PSA has led to the worst possible outcomes of overuse in men unlikely to benefit, high rates of overdiagnosis and overtreatment, and economic and racial inequity,” Dr. Vickers said. “Our view is that PSA screening should be done well — by implementing straightforward harm-reduction strategies like restricting screening in older men and use of secondary tests before biopsy — or not at all.”
Dr. James said that undertreatment of advanced disease is widespread; only about 30%-40% of men in the United States receive combination hormone therapy for metastatic disease, for example. “Simply doing what we know works would improve outcomes,” he said.
Dr. James said that men of African ancestry are twice as likely to develop prostate cancer, but whether treatment should follow a different approach in these men is unclear. The new report stressed the need to include more men of African ancestry in research.
Brandon Mahal, MD, vice chair of research in radiation oncology the University of Miami Sylvester Comprehensive Cancer Center and a coauthor of the report, said that new approaches are needed to enable earlier diagnosis of prostate cancer in men in low- to middle-income countries, where most patients present with metastatic disease and are less likely to survive for long periods.
Dr. James recommended pop-up clinics and mobile testing to encourage men who are at high risk for prostate cancer but feel well to detect lethal cancers early.
In England, for example, Dr. James helped introduce an outreach program called The Man Van which provided free health checks, including PSA tests, to high-risk men in London.
“By bringing a van with quick and easy testing straight to men at work and in the community, and targeting those who have a higher risk of prostate cancer, we provided thousands of health checks which resulted in almost 100 cancer diagnoses in men who might otherwise have only seen a doctor once their cancer has progressed to a more advanced stage,” he said.
He noted that the medical community worldwide is ill-prepared for the onslaught of prostate cancer cases.
“The solution cannot be training more urologists, radiation oncologists, pathologists, and radiologists because it simply takes too long,” Dr. James said. However, increased use of nurses and artificial intelligence may help. “In my own hospital, biopsies are a nurse-led and -delivered service. AI is extraordinarily good at diagnosis already and will only get better,” he said.
In poorer countries, smartphones could fill gaps too. “The same technology that does face recognition already can say that’s a Gleason 7 prostate cancer,” Dr. James said. “It’s not being rolled out in countries like America of course because pathologists’ income is at risk.”
Dr. James, Dr. Vickers, and Dr. Mahal reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
An “inevitable” global surge in prostate cancer is coming, with a worldwide doubling of cases to 2.9 million and an 85% increase in deaths to nearly 700,000 by the year 2040, the Lancet Commission on Prostate Cancer warned this week.
At a meeting of urologists in Paris, the commission said that the acceleration is already underway in high-income countries such as the United States and the United Kingdom but will gain momentum in low- and medium-income countries.
Nick James, MD, lead author of The Lancet report and professor of prostate and bladder cancer research at The Institute of Cancer Research in London, said that the surge, in part, is a medical success story.
Dr. James told this news organization.
“There is a big rise in the high-income countries. But we’re going to see a big rise in the number of 50-, 60-, 70-year-olds in the coming decades in the poorer countries, and with that comes more prostate cancer. High-income countries such as the UK and USA will also see smaller increases for the same reason.”
According to the report, to be presented April 6 at the 2024 European Association of Urology Congress in Paris, “The case for prostate cancer screening for all men aged 50-70 years (and all men of African origin aged 45–70 years) in high-income countries is strengthening with improved use of technologies such as MRI and growing evidence for the safety of active surveillance.”
Andrew Vickers, PhD, a biostatistician at Memorial Sloan Kettering Cancer Center in New York City, said that the Lancet Commission came to similar conclusions as he and an international group of researchers did in a 2023 policy paper in The BMJ. A major gap, Dr. Vickers said, is misuse of prostate-specific antigen (PSA) screening.
“We found that the ubiquitous policy compromise of letting patients decide for themselves about PSA has led to the worst possible outcomes of overuse in men unlikely to benefit, high rates of overdiagnosis and overtreatment, and economic and racial inequity,” Dr. Vickers said. “Our view is that PSA screening should be done well — by implementing straightforward harm-reduction strategies like restricting screening in older men and use of secondary tests before biopsy — or not at all.”
Dr. James said that undertreatment of advanced disease is widespread; only about 30%-40% of men in the United States receive combination hormone therapy for metastatic disease, for example. “Simply doing what we know works would improve outcomes,” he said.
Dr. James said that men of African ancestry are twice as likely to develop prostate cancer, but whether treatment should follow a different approach in these men is unclear. The new report stressed the need to include more men of African ancestry in research.
Brandon Mahal, MD, vice chair of research in radiation oncology the University of Miami Sylvester Comprehensive Cancer Center and a coauthor of the report, said that new approaches are needed to enable earlier diagnosis of prostate cancer in men in low- to middle-income countries, where most patients present with metastatic disease and are less likely to survive for long periods.
Dr. James recommended pop-up clinics and mobile testing to encourage men who are at high risk for prostate cancer but feel well to detect lethal cancers early.
In England, for example, Dr. James helped introduce an outreach program called The Man Van which provided free health checks, including PSA tests, to high-risk men in London.
“By bringing a van with quick and easy testing straight to men at work and in the community, and targeting those who have a higher risk of prostate cancer, we provided thousands of health checks which resulted in almost 100 cancer diagnoses in men who might otherwise have only seen a doctor once their cancer has progressed to a more advanced stage,” he said.
He noted that the medical community worldwide is ill-prepared for the onslaught of prostate cancer cases.
“The solution cannot be training more urologists, radiation oncologists, pathologists, and radiologists because it simply takes too long,” Dr. James said. However, increased use of nurses and artificial intelligence may help. “In my own hospital, biopsies are a nurse-led and -delivered service. AI is extraordinarily good at diagnosis already and will only get better,” he said.
In poorer countries, smartphones could fill gaps too. “The same technology that does face recognition already can say that’s a Gleason 7 prostate cancer,” Dr. James said. “It’s not being rolled out in countries like America of course because pathologists’ income is at risk.”
Dr. James, Dr. Vickers, and Dr. Mahal reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
An “inevitable” global surge in prostate cancer is coming, with a worldwide doubling of cases to 2.9 million and an 85% increase in deaths to nearly 700,000 by the year 2040, the Lancet Commission on Prostate Cancer warned this week.
At a meeting of urologists in Paris, the commission said that the acceleration is already underway in high-income countries such as the United States and the United Kingdom but will gain momentum in low- and medium-income countries.
Nick James, MD, lead author of The Lancet report and professor of prostate and bladder cancer research at The Institute of Cancer Research in London, said that the surge, in part, is a medical success story.
Dr. James told this news organization.
“There is a big rise in the high-income countries. But we’re going to see a big rise in the number of 50-, 60-, 70-year-olds in the coming decades in the poorer countries, and with that comes more prostate cancer. High-income countries such as the UK and USA will also see smaller increases for the same reason.”
According to the report, to be presented April 6 at the 2024 European Association of Urology Congress in Paris, “The case for prostate cancer screening for all men aged 50-70 years (and all men of African origin aged 45–70 years) in high-income countries is strengthening with improved use of technologies such as MRI and growing evidence for the safety of active surveillance.”
Andrew Vickers, PhD, a biostatistician at Memorial Sloan Kettering Cancer Center in New York City, said that the Lancet Commission came to similar conclusions as he and an international group of researchers did in a 2023 policy paper in The BMJ. A major gap, Dr. Vickers said, is misuse of prostate-specific antigen (PSA) screening.
“We found that the ubiquitous policy compromise of letting patients decide for themselves about PSA has led to the worst possible outcomes of overuse in men unlikely to benefit, high rates of overdiagnosis and overtreatment, and economic and racial inequity,” Dr. Vickers said. “Our view is that PSA screening should be done well — by implementing straightforward harm-reduction strategies like restricting screening in older men and use of secondary tests before biopsy — or not at all.”
Dr. James said that undertreatment of advanced disease is widespread; only about 30%-40% of men in the United States receive combination hormone therapy for metastatic disease, for example. “Simply doing what we know works would improve outcomes,” he said.
Dr. James said that men of African ancestry are twice as likely to develop prostate cancer, but whether treatment should follow a different approach in these men is unclear. The new report stressed the need to include more men of African ancestry in research.
Brandon Mahal, MD, vice chair of research in radiation oncology the University of Miami Sylvester Comprehensive Cancer Center and a coauthor of the report, said that new approaches are needed to enable earlier diagnosis of prostate cancer in men in low- to middle-income countries, where most patients present with metastatic disease and are less likely to survive for long periods.
Dr. James recommended pop-up clinics and mobile testing to encourage men who are at high risk for prostate cancer but feel well to detect lethal cancers early.
In England, for example, Dr. James helped introduce an outreach program called The Man Van which provided free health checks, including PSA tests, to high-risk men in London.
“By bringing a van with quick and easy testing straight to men at work and in the community, and targeting those who have a higher risk of prostate cancer, we provided thousands of health checks which resulted in almost 100 cancer diagnoses in men who might otherwise have only seen a doctor once their cancer has progressed to a more advanced stage,” he said.
He noted that the medical community worldwide is ill-prepared for the onslaught of prostate cancer cases.
“The solution cannot be training more urologists, radiation oncologists, pathologists, and radiologists because it simply takes too long,” Dr. James said. However, increased use of nurses and artificial intelligence may help. “In my own hospital, biopsies are a nurse-led and -delivered service. AI is extraordinarily good at diagnosis already and will only get better,” he said.
In poorer countries, smartphones could fill gaps too. “The same technology that does face recognition already can say that’s a Gleason 7 prostate cancer,” Dr. James said. “It’s not being rolled out in countries like America of course because pathologists’ income is at risk.”
Dr. James, Dr. Vickers, and Dr. Mahal reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
New Guidelines: Start PSA Screening Earlier in Black Men
Lowering the recommended age for baseline prostate-specific antigen (PSA) would reduce prostate cancer deaths by about 30% in Black men without significantly increasing the rate of overdiagnosis, according to new screening guidelines from the Prostate Cancer Foundation.
Specifically, , a multidisciplinary panel of experts and patient advocates determined based on a comprehensive literature review.
The panel’s findings were presented in a poster at the ASCO Genitourinary Cancers Symposium.
“Black men in the United States are considered a high-risk population for being diagnosed with and dying from prostate cancer,” wrote lead author Isla Garraway, MD, PhD, of the University of California, Los Angeles, and colleagues. Specifically, Black men are about two times more likely to be diagnosed with and die from prostate cancer than White men. But, the authors continued, “few guidelines have outlined specific recommendations for PSA-based prostate cancer screening among Black men.”
The US Preventive Services Task Force recommendations, which are currently being updated, set the PSA screening start age at 55. The task force recommendations, which dictate insurance coverage in the United States, acknowledged “a potential mortality benefit for African American men when beginning screening before age 55 years” but did not explicitly recommend screening earlier.
Current guidelines from the American Cancer Society call for discussions about screening in average-risk men to begin at age 50-55. The recommendations do specify lowering the age to 45 for those at a high risk for prostate cancer, which includes Black men as well as those with a first-degree relative diagnosed with prostate cancer before age 65. In some cases, screening can begin at age 40 in the highest risk men — those with more than one first-degree relative who had prostate cancer at a young age.
The Prostate Cancer Foundation “wanted to address the confusion around different guideline statements and the lack of clarity around screening recommendations for Black men,” said William K. Oh, MD, of The Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York City, who chaired the panel for the new guidelines. “We thus convened a distinguished panel of experts from diverse backgrounds and expertise to create six guidelines statements to help Black men, their families, and their healthcare providers to consider options for prostate cancer screening based on the best available evidence.”
After reviewing 287, the expert panel developed six new guideline statements, reaching at least 80% consensus among panel members, addressing screening for Black men:
{kind=link}
- Because Black men are at a high risk for prostate cancer, the benefits of screening generally outweigh the risks.
- PSA testing should be considered first line for prostate cancer screening, although some providers may recommend an optional digital rectal exam in addition to the PSA test.
- Black men should engage in shared decision-making with their healthcare providers and other trusted sources of information to learn about the pros and cons of screening.
- For Black men who elect screening, a baseline PSA test should be done between ages 40 and 45, and annual PSA screening should be strongly considered based on the PSA value and the individual’s health status.
- Black men over age 70 who have been undergoing prostate cancer screening should talk with their healthcare provider about whether to continue PSA testing and make an informed decision based on their age, life expectancy, health status, family history, and prior PSA levels.
- Black men who are at even higher risk due to a strong family history and/or known carriers of high-risk genetic variants should consider initiating annual PSA screening as early as age 40.
These statements are based on “the best available evidence, which overwhelmingly supports the conclusion that Black men in the US could benefit from a risk-adapted PSA screening,” the investigators concluded, noting that the latest evidence “warrants revisiting current recommendations for early [prostate cancer] detection in Black men from other national guideline groups.”
“We believe that the outcome of these more directed guidelines will be to give clarity to these men,” added Oh, who is also chief medical officer for the Prostate Cancer Foundation.
This research was funded by the Prostate Cancer Foundation, National Cancer Institute, Veterans Affairs, Jean Perkins Foundation, and Department of Defense. Garraway reported having no disclosures.
A version of this article appeared on Medscape.com.
Lowering the recommended age for baseline prostate-specific antigen (PSA) would reduce prostate cancer deaths by about 30% in Black men without significantly increasing the rate of overdiagnosis, according to new screening guidelines from the Prostate Cancer Foundation.
Specifically, , a multidisciplinary panel of experts and patient advocates determined based on a comprehensive literature review.
The panel’s findings were presented in a poster at the ASCO Genitourinary Cancers Symposium.
“Black men in the United States are considered a high-risk population for being diagnosed with and dying from prostate cancer,” wrote lead author Isla Garraway, MD, PhD, of the University of California, Los Angeles, and colleagues. Specifically, Black men are about two times more likely to be diagnosed with and die from prostate cancer than White men. But, the authors continued, “few guidelines have outlined specific recommendations for PSA-based prostate cancer screening among Black men.”
The US Preventive Services Task Force recommendations, which are currently being updated, set the PSA screening start age at 55. The task force recommendations, which dictate insurance coverage in the United States, acknowledged “a potential mortality benefit for African American men when beginning screening before age 55 years” but did not explicitly recommend screening earlier.
Current guidelines from the American Cancer Society call for discussions about screening in average-risk men to begin at age 50-55. The recommendations do specify lowering the age to 45 for those at a high risk for prostate cancer, which includes Black men as well as those with a first-degree relative diagnosed with prostate cancer before age 65. In some cases, screening can begin at age 40 in the highest risk men — those with more than one first-degree relative who had prostate cancer at a young age.
The Prostate Cancer Foundation “wanted to address the confusion around different guideline statements and the lack of clarity around screening recommendations for Black men,” said William K. Oh, MD, of The Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York City, who chaired the panel for the new guidelines. “We thus convened a distinguished panel of experts from diverse backgrounds and expertise to create six guidelines statements to help Black men, their families, and their healthcare providers to consider options for prostate cancer screening based on the best available evidence.”
After reviewing 287, the expert panel developed six new guideline statements, reaching at least 80% consensus among panel members, addressing screening for Black men:
- Because Black men are at a high risk for prostate cancer, the benefits of screening generally outweigh the risks.
- PSA testing should be considered first line for prostate cancer screening, although some providers may recommend an optional digital rectal exam in addition to the PSA test.
- Black men should engage in shared decision-making with their healthcare providers and other trusted sources of information to learn about the pros and cons of screening.
- For Black men who elect screening, a baseline PSA test should be done between ages 40 and 45, and annual PSA screening should be strongly considered based on the PSA value and the individual’s health status.
- Black men over age 70 who have been undergoing prostate cancer screening should talk with their healthcare provider about whether to continue PSA testing and make an informed decision based on their age, life expectancy, health status, family history, and prior PSA levels.
- Black men who are at even higher risk due to a strong family history and/or known carriers of high-risk genetic variants should consider initiating annual PSA screening as early as age 40.
These statements are based on “the best available evidence, which overwhelmingly supports the conclusion that Black men in the US could benefit from a risk-adapted PSA screening,” the investigators concluded, noting that the latest evidence “warrants revisiting current recommendations for early [prostate cancer] detection in Black men from other national guideline groups.”
“We believe that the outcome of these more directed guidelines will be to give clarity to these men,” added Oh, who is also chief medical officer for the Prostate Cancer Foundation.
This research was funded by the Prostate Cancer Foundation, National Cancer Institute, Veterans Affairs, Jean Perkins Foundation, and Department of Defense. Garraway reported having no disclosures.
A version of this article appeared on Medscape.com.
Lowering the recommended age for baseline prostate-specific antigen (PSA) would reduce prostate cancer deaths by about 30% in Black men without significantly increasing the rate of overdiagnosis, according to new screening guidelines from the Prostate Cancer Foundation.
Specifically, , a multidisciplinary panel of experts and patient advocates determined based on a comprehensive literature review.
The panel’s findings were presented in a poster at the ASCO Genitourinary Cancers Symposium.
“Black men in the United States are considered a high-risk population for being diagnosed with and dying from prostate cancer,” wrote lead author Isla Garraway, MD, PhD, of the University of California, Los Angeles, and colleagues. Specifically, Black men are about two times more likely to be diagnosed with and die from prostate cancer than White men. But, the authors continued, “few guidelines have outlined specific recommendations for PSA-based prostate cancer screening among Black men.”
The US Preventive Services Task Force recommendations, which are currently being updated, set the PSA screening start age at 55. The task force recommendations, which dictate insurance coverage in the United States, acknowledged “a potential mortality benefit for African American men when beginning screening before age 55 years” but did not explicitly recommend screening earlier.
Current guidelines from the American Cancer Society call for discussions about screening in average-risk men to begin at age 50-55. The recommendations do specify lowering the age to 45 for those at a high risk for prostate cancer, which includes Black men as well as those with a first-degree relative diagnosed with prostate cancer before age 65. In some cases, screening can begin at age 40 in the highest risk men — those with more than one first-degree relative who had prostate cancer at a young age.
The Prostate Cancer Foundation “wanted to address the confusion around different guideline statements and the lack of clarity around screening recommendations for Black men,” said William K. Oh, MD, of The Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York City, who chaired the panel for the new guidelines. “We thus convened a distinguished panel of experts from diverse backgrounds and expertise to create six guidelines statements to help Black men, their families, and their healthcare providers to consider options for prostate cancer screening based on the best available evidence.”
After reviewing 287, the expert panel developed six new guideline statements, reaching at least 80% consensus among panel members, addressing screening for Black men:
- Because Black men are at a high risk for prostate cancer, the benefits of screening generally outweigh the risks.
- PSA testing should be considered first line for prostate cancer screening, although some providers may recommend an optional digital rectal exam in addition to the PSA test.
- Black men should engage in shared decision-making with their healthcare providers and other trusted sources of information to learn about the pros and cons of screening.
- For Black men who elect screening, a baseline PSA test should be done between ages 40 and 45, and annual PSA screening should be strongly considered based on the PSA value and the individual’s health status.
- Black men over age 70 who have been undergoing prostate cancer screening should talk with their healthcare provider about whether to continue PSA testing and make an informed decision based on their age, life expectancy, health status, family history, and prior PSA levels.
- Black men who are at even higher risk due to a strong family history and/or known carriers of high-risk genetic variants should consider initiating annual PSA screening as early as age 40.
These statements are based on “the best available evidence, which overwhelmingly supports the conclusion that Black men in the US could benefit from a risk-adapted PSA screening,” the investigators concluded, noting that the latest evidence “warrants revisiting current recommendations for early [prostate cancer] detection in Black men from other national guideline groups.”
“We believe that the outcome of these more directed guidelines will be to give clarity to these men,” added Oh, who is also chief medical officer for the Prostate Cancer Foundation.
This research was funded by the Prostate Cancer Foundation, National Cancer Institute, Veterans Affairs, Jean Perkins Foundation, and Department of Defense. Garraway reported having no disclosures.
A version of this article appeared on Medscape.com.
FROM ASCO GU 2024
Cancer Data Trends 2024

The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
Click to view the Digital Edition.
In this issue:
Hepatocellular Carcinoma
Special care for veterans, changes in staging, and biomarkers for early diagnosis
Lung Cancer
Guideline updates and racial disparities in veterans
Multiple Myeloma
Improving survival in the VA
Colorectal Cancer
Barriers to follow-up colonoscopies after FIT testing
B-Cell Lymphomas
Findings from the VA's National TeleOncology Program and recent therapy updates
Breast Cancer
A look at the VA's Risk Assessment Pipeline and incidence among veterans vs the general population
Genitourinary Cancers
Molecular testing in prostate cancer, improving survival for metastatic RCC, and links between bladder cancer and Agent Orange exposure
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
Click to view the Digital Edition.
In this issue:
Hepatocellular Carcinoma
Special care for veterans, changes in staging, and biomarkers for early diagnosis
Lung Cancer
Guideline updates and racial disparities in veterans
Multiple Myeloma
Improving survival in the VA
Colorectal Cancer
Barriers to follow-up colonoscopies after FIT testing
B-Cell Lymphomas
Findings from the VA's National TeleOncology Program and recent therapy updates
Breast Cancer
A look at the VA's Risk Assessment Pipeline and incidence among veterans vs the general population
Genitourinary Cancers
Molecular testing in prostate cancer, improving survival for metastatic RCC, and links between bladder cancer and Agent Orange exposure
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
Click to view the Digital Edition.
In this issue:
Hepatocellular Carcinoma
Special care for veterans, changes in staging, and biomarkers for early diagnosis
Lung Cancer
Guideline updates and racial disparities in veterans
Multiple Myeloma
Improving survival in the VA
Colorectal Cancer
Barriers to follow-up colonoscopies after FIT testing
B-Cell Lymphomas
Findings from the VA's National TeleOncology Program and recent therapy updates
Breast Cancer
A look at the VA's Risk Assessment Pipeline and incidence among veterans vs the general population
Genitourinary Cancers
Molecular testing in prostate cancer, improving survival for metastatic RCC, and links between bladder cancer and Agent Orange exposure
Cancer Data Trends 2024: Genitourinary Cancers
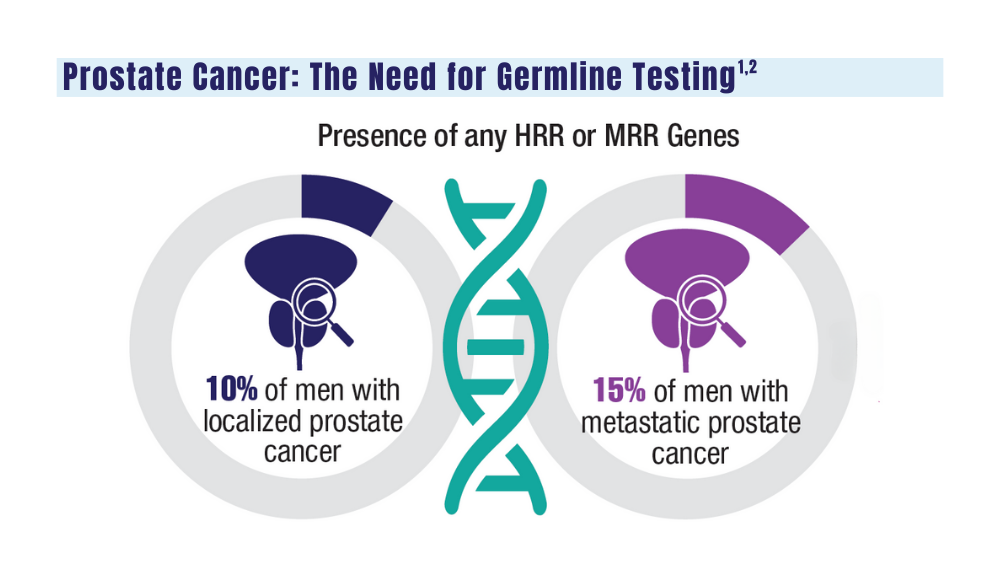
1. Sokolova A, Cheng H. Germline testing in prostate cancer: when and who to test. Oncology (Williston Park). 2021;35(10):645-653. doi:10.46883/ONC.2021.3510.0645
2. Tuffaha H, Edmunds K, Fairbairn D, et al. Guidelines for genetic testing in prostate cancer: a scoping review. Prostate Cancer Prostatic Dis. 2023 May 18. doi:10.1038/s41391-023-00676-0
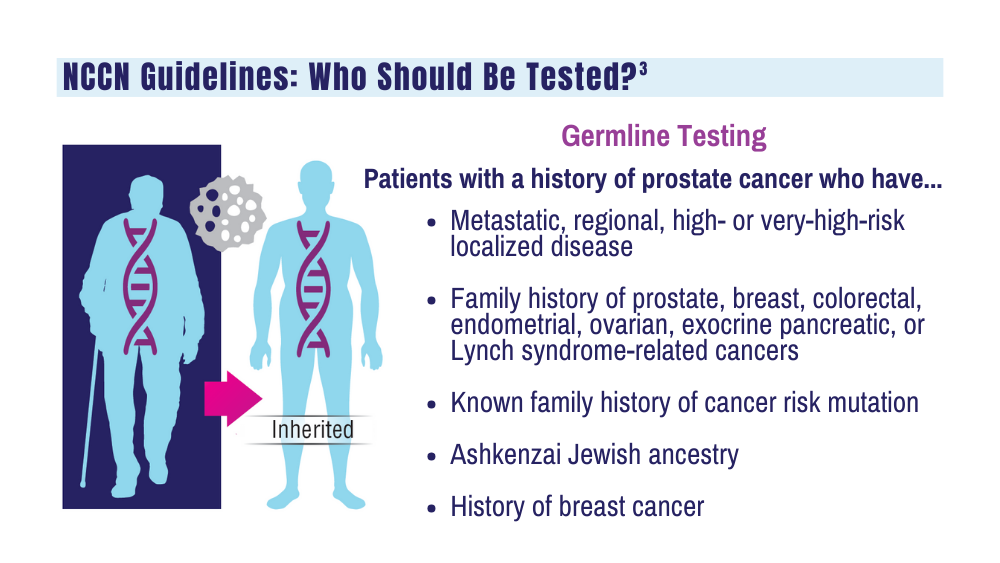
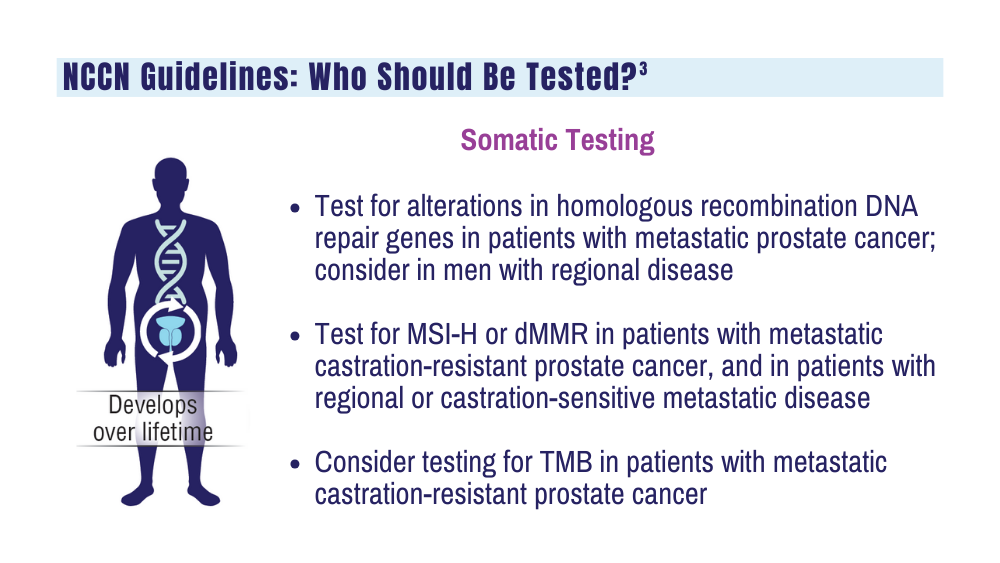
3. National Comprehensive Cancer Network. NCCN clinical practice guidelines for prostate cancer. Version 4.2023. September 7, 2023. Accessed December 20, 2023. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
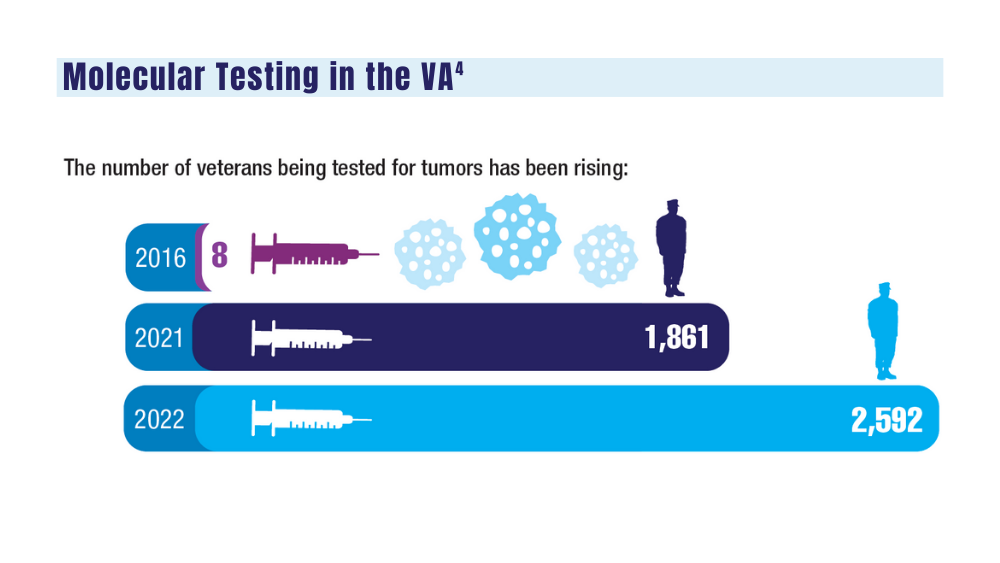
4. National Precision Oncology Program. PMID 26149669 (e-mail, December 13, 2023).
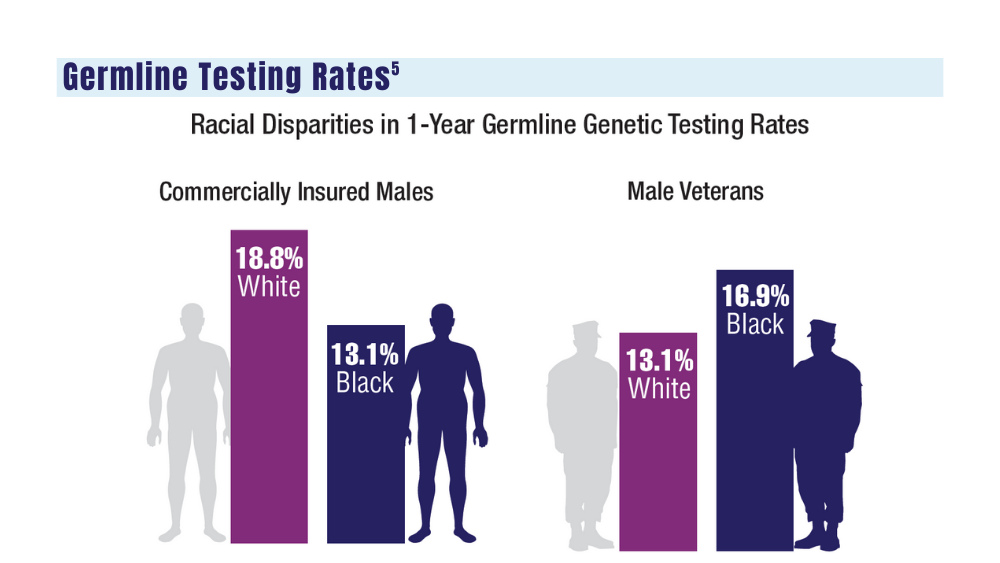
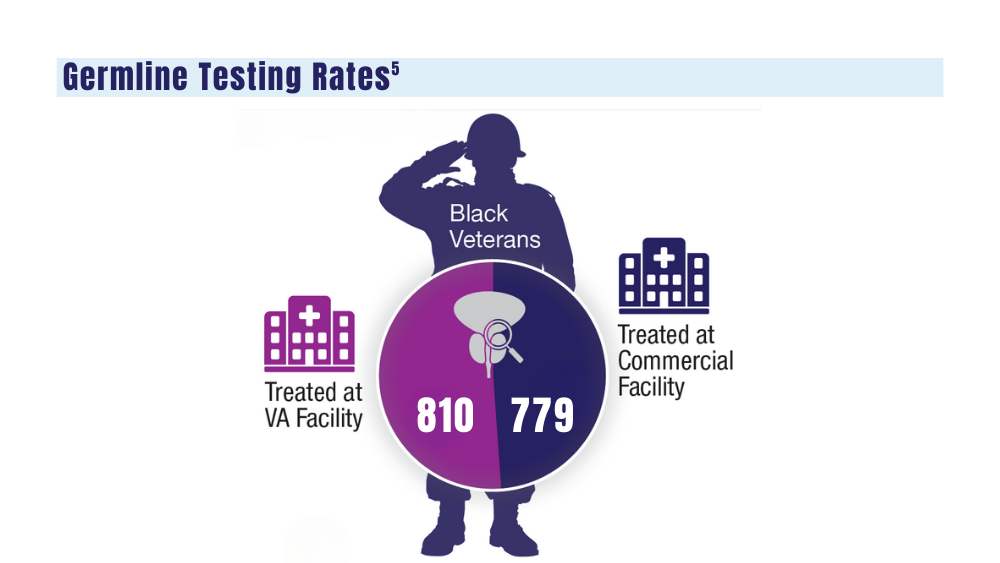
5. Shevach J, Lynch J, Candelieri-Surette D, et al. Racial disparities in germline testing among men with pancreas, breast and metastatic prostate cancers in two health systems. J Clin Oncol. 2023;41(16 suppl):abstract 10549. https://ascopubs.org/doi/abs/10.1200/JCO.2023.41.16_suppl.10549
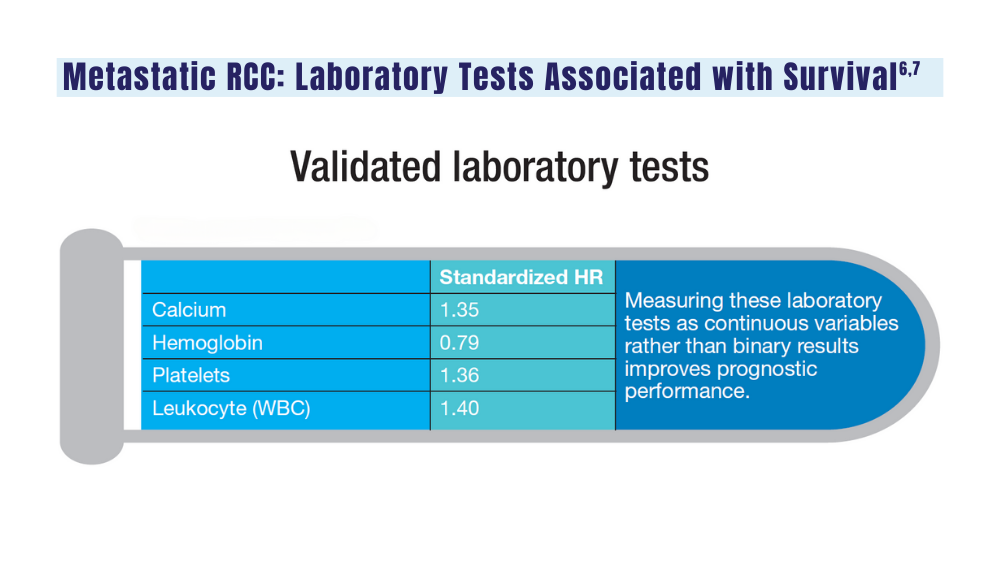
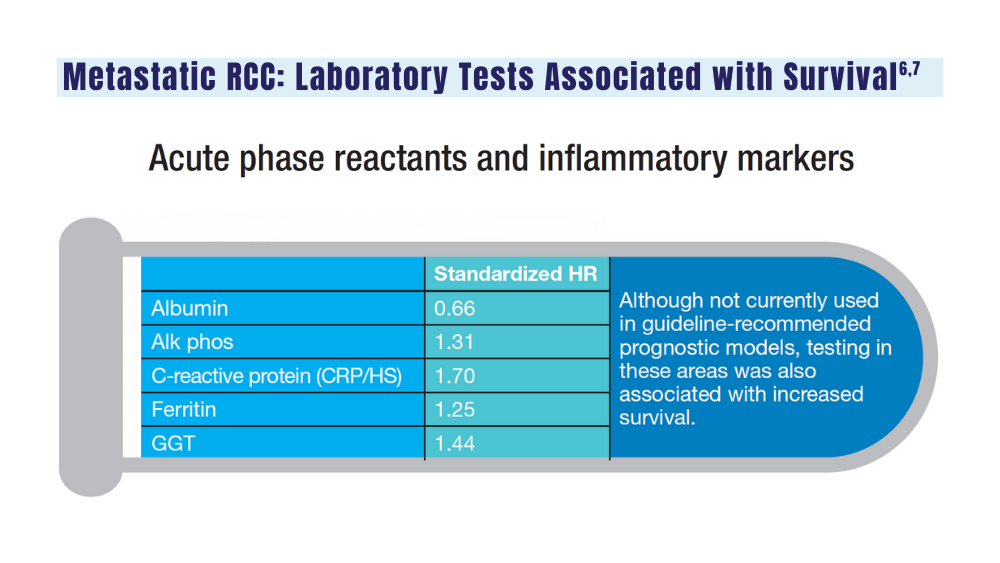
6. Velaer K, Thomas IC, Yang J, et al. Clinical laboratory tests associated with survival in patients with metastatic renal cell carcinoma: a laboratory wide association study (LWAS). Urol Oncol. 2022;40(1):12.e23-12.e30. doi:10.1016/j.urolonc.2021.08.011
7. Heng DYC, Xie W, Regan MM, et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. Lancet Oncol. 2013;14(2):141-148. doi:10.1016/S1470-2045(12)70559-4
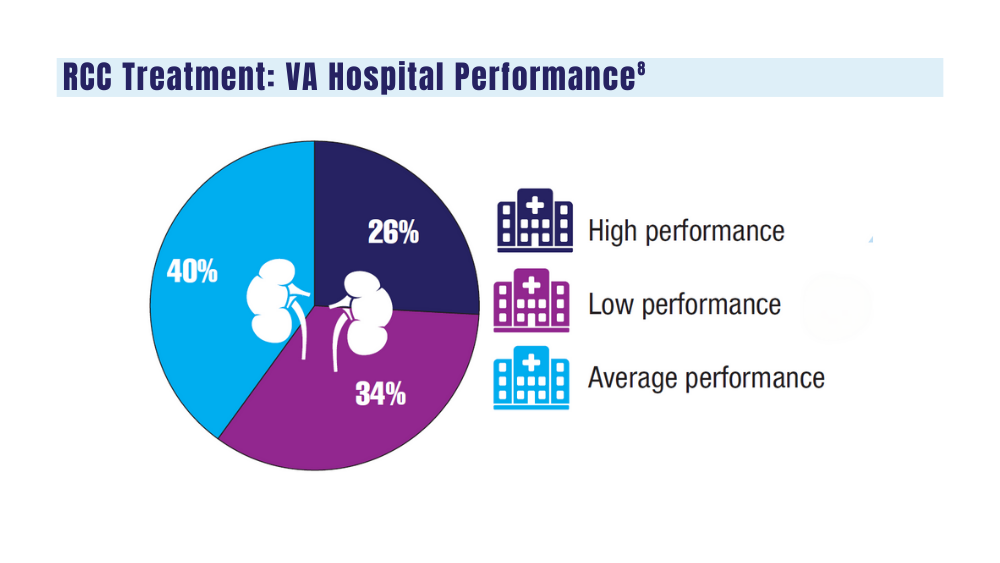
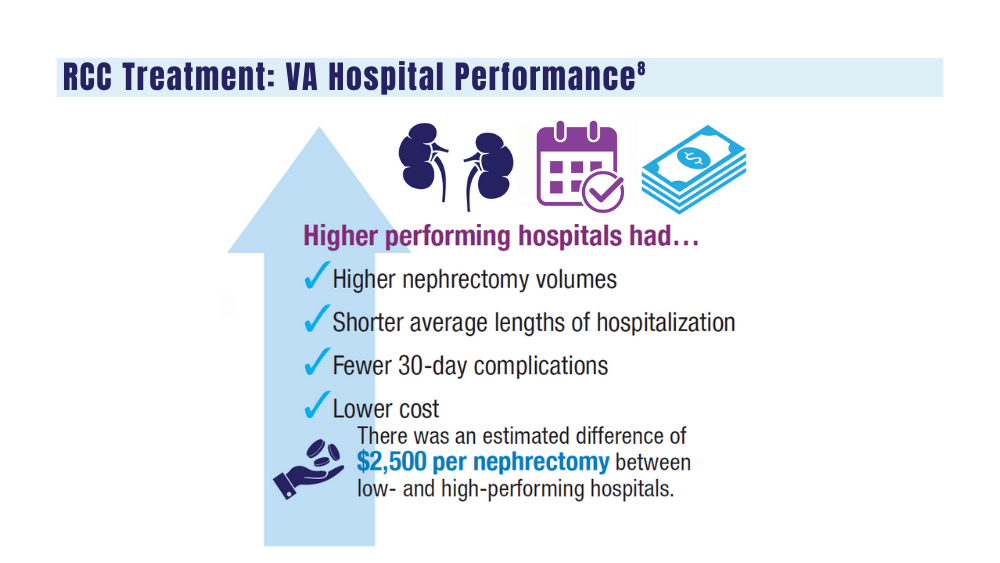
8. Aguilar Palacios D, Wilson B, Michael P, et al. A novel metric for hospital quality in kidney cancer surgery: a Veterans Affairs National Health System validation of concept. Urol Pract. 2022;9(3):237-245. doi:10.1097/UPJ.0000000000000294
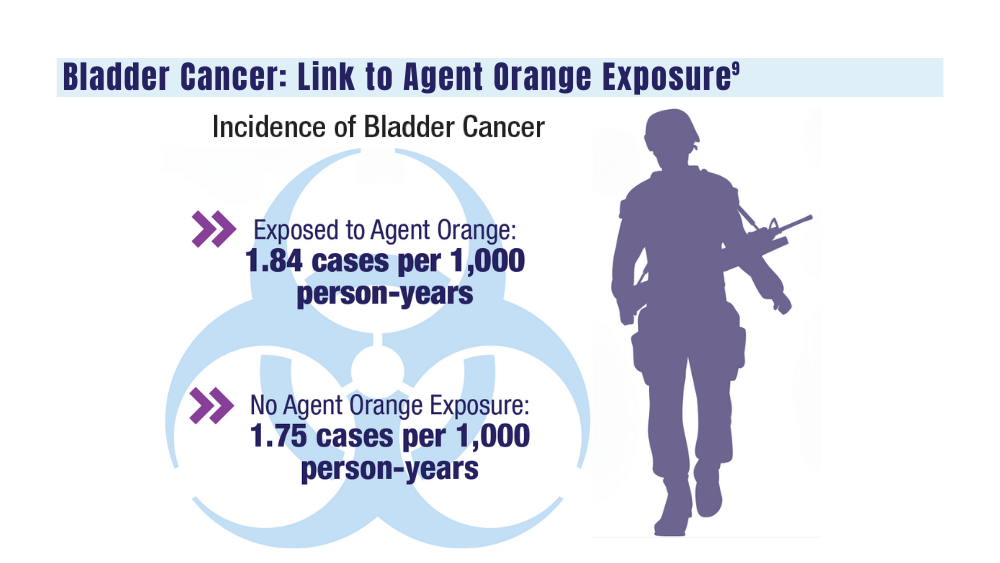
9. Williams SB, Janes JL, Howard LE, et al. Exposure to Agent Orange and risk of bladder cancer among US veterans. JAMA Netw Open. 2023;6(6):e2320593. doi:10.1001/jamanetworkopen.2023.20593
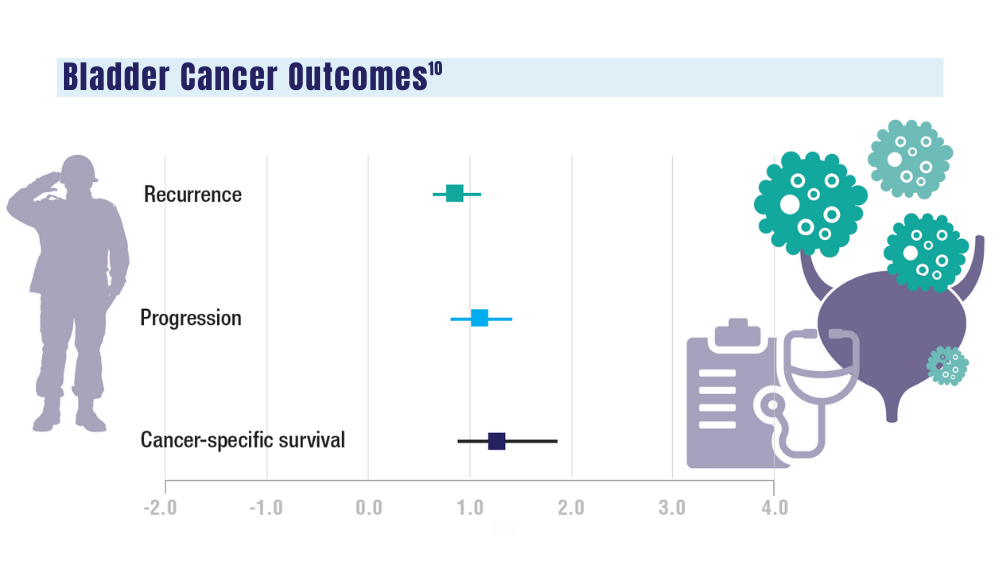
10. Penn T, Borza T, Liou JI, et al. Impact of Agent Orange exposure on non-muscle invasive bladder cancer outcomes. Urology. 2023;182:175-180. doi:10.1016/j.urology.2023.08.037
1. Sokolova A, Cheng H. Germline testing in prostate cancer: when and who to test. Oncology (Williston Park). 2021;35(10):645-653. doi:10.46883/ONC.2021.3510.0645
2. Tuffaha H, Edmunds K, Fairbairn D, et al. Guidelines for genetic testing in prostate cancer: a scoping review. Prostate Cancer Prostatic Dis. 2023 May 18. doi:10.1038/s41391-023-00676-0
3. National Comprehensive Cancer Network. NCCN clinical practice guidelines for prostate cancer. Version 4.2023. September 7, 2023. Accessed December 20, 2023. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
4. National Precision Oncology Program. PMID 26149669 (e-mail, December 13, 2023).
5. Shevach J, Lynch J, Candelieri-Surette D, et al. Racial disparities in germline testing among men with pancreas, breast and metastatic prostate cancers in two health systems. J Clin Oncol. 2023;41(16 suppl):abstract 10549. https://ascopubs.org/doi/abs/10.1200/JCO.2023.41.16_suppl.10549
6. Velaer K, Thomas IC, Yang J, et al. Clinical laboratory tests associated with survival in patients with metastatic renal cell carcinoma: a laboratory wide association study (LWAS). Urol Oncol. 2022;40(1):12.e23-12.e30. doi:10.1016/j.urolonc.2021.08.011
7. Heng DYC, Xie W, Regan MM, et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. Lancet Oncol. 2013;14(2):141-148. doi:10.1016/S1470-2045(12)70559-4
8. Aguilar Palacios D, Wilson B, Michael P, et al. A novel metric for hospital quality in kidney cancer surgery: a Veterans Affairs National Health System validation of concept. Urol Pract. 2022;9(3):237-245. doi:10.1097/UPJ.0000000000000294
9. Williams SB, Janes JL, Howard LE, et al. Exposure to Agent Orange and risk of bladder cancer among US veterans. JAMA Netw Open. 2023;6(6):e2320593. doi:10.1001/jamanetworkopen.2023.20593
10. Penn T, Borza T, Liou JI, et al. Impact of Agent Orange exposure on non-muscle invasive bladder cancer outcomes. Urology. 2023;182:175-180. doi:10.1016/j.urology.2023.08.037
1. Sokolova A, Cheng H. Germline testing in prostate cancer: when and who to test. Oncology (Williston Park). 2021;35(10):645-653. doi:10.46883/ONC.2021.3510.0645
2. Tuffaha H, Edmunds K, Fairbairn D, et al. Guidelines for genetic testing in prostate cancer: a scoping review. Prostate Cancer Prostatic Dis. 2023 May 18. doi:10.1038/s41391-023-00676-0
3. National Comprehensive Cancer Network. NCCN clinical practice guidelines for prostate cancer. Version 4.2023. September 7, 2023. Accessed December 20, 2023. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
4. National Precision Oncology Program. PMID 26149669 (e-mail, December 13, 2023).
5. Shevach J, Lynch J, Candelieri-Surette D, et al. Racial disparities in germline testing among men with pancreas, breast and metastatic prostate cancers in two health systems. J Clin Oncol. 2023;41(16 suppl):abstract 10549. https://ascopubs.org/doi/abs/10.1200/JCO.2023.41.16_suppl.10549
6. Velaer K, Thomas IC, Yang J, et al. Clinical laboratory tests associated with survival in patients with metastatic renal cell carcinoma: a laboratory wide association study (LWAS). Urol Oncol. 2022;40(1):12.e23-12.e30. doi:10.1016/j.urolonc.2021.08.011
7. Heng DYC, Xie W, Regan MM, et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. Lancet Oncol. 2013;14(2):141-148. doi:10.1016/S1470-2045(12)70559-4
8. Aguilar Palacios D, Wilson B, Michael P, et al. A novel metric for hospital quality in kidney cancer surgery: a Veterans Affairs National Health System validation of concept. Urol Pract. 2022;9(3):237-245. doi:10.1097/UPJ.0000000000000294
9. Williams SB, Janes JL, Howard LE, et al. Exposure to Agent Orange and risk of bladder cancer among US veterans. JAMA Netw Open. 2023;6(6):e2320593. doi:10.1001/jamanetworkopen.2023.20593
10. Penn T, Borza T, Liou JI, et al. Impact of Agent Orange exposure on non-muscle invasive bladder cancer outcomes. Urology. 2023;182:175-180. doi:10.1016/j.urology.2023.08.037
Higher Prostate Cancer Rates Seen in Black Men, but Advanced Cases Similar to White Men
There was a substantial difference in prostate cancer diagnosis across ethnic groups: 25% of Black men with a raised PSA were diagnosed with prostate cancer within 1 year of being tested, compared with 20% of White men and 13% of Asian men, in the analysis of a large primary care cohort in the United Kingdom.
Incidence of advanced prostate cancer for Asian men with a raised PSA result was 4.5%, compared with 7.5% for White men and 7.0% for Black men.
Men included in the study were aged 40 and older and had no prior cancer diagnosis. Their ethnicity and PSA test result were logged in a national dataset between 2010 and 2017.
The study of more than 730,000 men, published in BMC Medicine, didn’t explore reasons for the differences, but experts offer their thoughts on what led to the findings and what these results imply.
Why the Higher Diagnosis Rates but Not More Advanced Disease in Black Men?
Lead author Liz Down, a graduate research assistant at the University of Exeter, Exeter, England, suggests the higher diagnosis rates but not more advanced disease in Black men may be linked to genetic variations.
Her team’s studies have shown that Black men in the United Kingdom and United States have higher levels of PSA. The PSA value is used to identify patients who might benefit from specialist investigation, and current guidelines in the UK and US don’t distinguish between ethnic groups.
As most men have slow-growing prostate cancer, this may lead to a disproportionately higher number of Black men being diagnosed with prostate cancer, she said.
“One possible interpretation,” Ms. Down notes, “is that prostate cancer follows a similar trajectory in Black and White men. What is different, however, is that Black men have higher PSA levels.”
As to why the advanced-cancer incidence is similar in Black and White patients in the study, Daniel George, MD, director of genitourinary oncology at Duke Cancer Institute in Durham, North Carolina, says it’s important to understand that the Black men in this study “are not necessarily representative of the Black population at large.”
In this study, “they’re a little bit more healthcare inclined,” Dr. George notes. The study population is actively seeking the PSA test. Their socioeconomic profile might be closer to their White counterparts’, and that may make results more similar, he said.
“It’s possible that because this is a screening and not just men coming in for symptoms or cause, that we’re not seeing as much advanced disease,” he continued.
Amar Kishan, MD, chief of the genitourinary oncology service at University of California Los Angeles (UCLA) Health, says the genomic factors and environmental stressors that lead to elevated PSA counts don’t necessarily translate into aggressiveness of disease.
Why do Different Races have Different Prostate Cancer Risk?
Dr. George points out that the study also highlights that Asian men were significantly less likely to be diagnosed with prostate cancer within 1 year of the test.
The reasons for differences in prostate risk by race are complex, he notes. There are some clues that biologic factors may be at work. For instance, early puberty has a link to prostate cancer as it does to breast cancer, and height is also associated with a greater risk of prostate cancer, Dr. George said.
It’s not necessarily a racial association but there are some biological factors associated with prostate cancer later in life, he explained. “These may be enriched in certain populations, including northern Europeans and patients with African ancestries.”
The study also notes that Black men are more likely to die from prostate cancer than are White men, and Asian men are less likely than White or Black men to die from it.
Ms. Down said the difference in prostate cancer mortality between Black vs White men, in particular, may be related to a number of factors, and age, and lifetime risk of prostate cancer may play a major role, at least in the UK.
Should There Be Different ‘Normal’ PSA Levels for Different Races?
Dr. George says there is likely a need to change the system because a PSA level in one race may not signal the same risk it does in another. So medicine probably needs to standardize what a “normal” PSA is by race, he says, adding that he is a coauthor of an upcoming paper regarding that issue.
The lowest instances of prostate cancer were in Asian patients so this isn’t just a Black and White issue, Dr. George notes. “Being able to establish benchmarks by race and ethnicity is something that is probably needed in the field,” he says.
Dr. Kishan, on the other hand, says data from this study are not enough to support differentiating PSA levels based on race. He noted a limitation of the study is that it was not able to calculate the false-negative rate of PSA tests.
What are the Implications for Treating and Screening for Prostate Cancer
Dr. Kishan says there may be a role for increased intensity of screening, whether at an earlier age or with different intervals, but prostate cancer treatment should not differ by race.
“Our prior study, as well as others,” he says, “have shown that when you balance Black and White patients for every factor that might impact prognosis other than race — such as age, disease aggressiveness, etc. — Black men actually tend to have better outcomes than White men. Thus, it would mean potentially overtreating (i.e., causing unnecessary side effects) to increase treatment intensity purely based on race with the available data.”
According to the paper, prostate cancer incidence in men with higher PSA levels increases with increasing age, even when using age-adjusted thresholds.
Dr. George says we know from this study and other studies as well that Black men are more likely to be diagnosed with prostate at a younger age. “Therefore, we probably need to be thinking about screening Black men starting at a younger age. These are the men who are most likely to benefit from an intervention — patients who have life expectancies of 20 years or more.”
What are the Downsides to Overdiagnosing Prostate Cancer in Men?
“It’s one of the biggest concerns that men have in proactively seeking healthcare,” Dr. George says. “They’re more likely to undergo treatment for this disease if they’re getting screened because (clinicians are) more likely to find it.”
Some of those men, he says, are going to undergo treatment for disease that won’t ultimately kill them, but may cause complications the men shouldn’t have had at all or otherwise may have had later.
“Overtreatment is a real concern. That’s why active surveillance is so important to minimize overtreatment of patients by finding out which cancers are low risk for progression and which are becoming more aggressive,” Dr. George says.
Authors of the study write that “the potential for overdiagnosis and the subsequent psychological and physical impact of diagnosis and treatment is an important consideration.”
All authors of the new paper received financial support from Cancer Research UK, the National Institute for Health and Care Research (NIHR), and the Higgins family for the submitted work.
Dr. George reports no relevant financial relationships.
Dr. Kishan reports consulting fees and speaking honoraria from Varian Medical Systems, Janssen, and Boston Scientific; research funding from PointBioPharma, Lantheus, and Janssen; and serving on advisory boards for Lantheus, Janssen and Boston Scientific.
There was a substantial difference in prostate cancer diagnosis across ethnic groups: 25% of Black men with a raised PSA were diagnosed with prostate cancer within 1 year of being tested, compared with 20% of White men and 13% of Asian men, in the analysis of a large primary care cohort in the United Kingdom.
Incidence of advanced prostate cancer for Asian men with a raised PSA result was 4.5%, compared with 7.5% for White men and 7.0% for Black men.
Men included in the study were aged 40 and older and had no prior cancer diagnosis. Their ethnicity and PSA test result were logged in a national dataset between 2010 and 2017.
The study of more than 730,000 men, published in BMC Medicine, didn’t explore reasons for the differences, but experts offer their thoughts on what led to the findings and what these results imply.
Why the Higher Diagnosis Rates but Not More Advanced Disease in Black Men?
Lead author Liz Down, a graduate research assistant at the University of Exeter, Exeter, England, suggests the higher diagnosis rates but not more advanced disease in Black men may be linked to genetic variations.
Her team’s studies have shown that Black men in the United Kingdom and United States have higher levels of PSA. The PSA value is used to identify patients who might benefit from specialist investigation, and current guidelines in the UK and US don’t distinguish between ethnic groups.
As most men have slow-growing prostate cancer, this may lead to a disproportionately higher number of Black men being diagnosed with prostate cancer, she said.
“One possible interpretation,” Ms. Down notes, “is that prostate cancer follows a similar trajectory in Black and White men. What is different, however, is that Black men have higher PSA levels.”
As to why the advanced-cancer incidence is similar in Black and White patients in the study, Daniel George, MD, director of genitourinary oncology at Duke Cancer Institute in Durham, North Carolina, says it’s important to understand that the Black men in this study “are not necessarily representative of the Black population at large.”
In this study, “they’re a little bit more healthcare inclined,” Dr. George notes. The study population is actively seeking the PSA test. Their socioeconomic profile might be closer to their White counterparts’, and that may make results more similar, he said.
“It’s possible that because this is a screening and not just men coming in for symptoms or cause, that we’re not seeing as much advanced disease,” he continued.
Amar Kishan, MD, chief of the genitourinary oncology service at University of California Los Angeles (UCLA) Health, says the genomic factors and environmental stressors that lead to elevated PSA counts don’t necessarily translate into aggressiveness of disease.
Why do Different Races have Different Prostate Cancer Risk?
Dr. George points out that the study also highlights that Asian men were significantly less likely to be diagnosed with prostate cancer within 1 year of the test.
The reasons for differences in prostate risk by race are complex, he notes. There are some clues that biologic factors may be at work. For instance, early puberty has a link to prostate cancer as it does to breast cancer, and height is also associated with a greater risk of prostate cancer, Dr. George said.
It’s not necessarily a racial association but there are some biological factors associated with prostate cancer later in life, he explained. “These may be enriched in certain populations, including northern Europeans and patients with African ancestries.”
The study also notes that Black men are more likely to die from prostate cancer than are White men, and Asian men are less likely than White or Black men to die from it.
Ms. Down said the difference in prostate cancer mortality between Black vs White men, in particular, may be related to a number of factors, and age, and lifetime risk of prostate cancer may play a major role, at least in the UK.
Should There Be Different ‘Normal’ PSA Levels for Different Races?
Dr. George says there is likely a need to change the system because a PSA level in one race may not signal the same risk it does in another. So medicine probably needs to standardize what a “normal” PSA is by race, he says, adding that he is a coauthor of an upcoming paper regarding that issue.
The lowest instances of prostate cancer were in Asian patients so this isn’t just a Black and White issue, Dr. George notes. “Being able to establish benchmarks by race and ethnicity is something that is probably needed in the field,” he says.
Dr. Kishan, on the other hand, says data from this study are not enough to support differentiating PSA levels based on race. He noted a limitation of the study is that it was not able to calculate the false-negative rate of PSA tests.
What are the Implications for Treating and Screening for Prostate Cancer
Dr. Kishan says there may be a role for increased intensity of screening, whether at an earlier age or with different intervals, but prostate cancer treatment should not differ by race.
“Our prior study, as well as others,” he says, “have shown that when you balance Black and White patients for every factor that might impact prognosis other than race — such as age, disease aggressiveness, etc. — Black men actually tend to have better outcomes than White men. Thus, it would mean potentially overtreating (i.e., causing unnecessary side effects) to increase treatment intensity purely based on race with the available data.”
According to the paper, prostate cancer incidence in men with higher PSA levels increases with increasing age, even when using age-adjusted thresholds.
Dr. George says we know from this study and other studies as well that Black men are more likely to be diagnosed with prostate at a younger age. “Therefore, we probably need to be thinking about screening Black men starting at a younger age. These are the men who are most likely to benefit from an intervention — patients who have life expectancies of 20 years or more.”
What are the Downsides to Overdiagnosing Prostate Cancer in Men?
“It’s one of the biggest concerns that men have in proactively seeking healthcare,” Dr. George says. “They’re more likely to undergo treatment for this disease if they’re getting screened because (clinicians are) more likely to find it.”
Some of those men, he says, are going to undergo treatment for disease that won’t ultimately kill them, but may cause complications the men shouldn’t have had at all or otherwise may have had later.
“Overtreatment is a real concern. That’s why active surveillance is so important to minimize overtreatment of patients by finding out which cancers are low risk for progression and which are becoming more aggressive,” Dr. George says.
Authors of the study write that “the potential for overdiagnosis and the subsequent psychological and physical impact of diagnosis and treatment is an important consideration.”
All authors of the new paper received financial support from Cancer Research UK, the National Institute for Health and Care Research (NIHR), and the Higgins family for the submitted work.
Dr. George reports no relevant financial relationships.
Dr. Kishan reports consulting fees and speaking honoraria from Varian Medical Systems, Janssen, and Boston Scientific; research funding from PointBioPharma, Lantheus, and Janssen; and serving on advisory boards for Lantheus, Janssen and Boston Scientific.
There was a substantial difference in prostate cancer diagnosis across ethnic groups: 25% of Black men with a raised PSA were diagnosed with prostate cancer within 1 year of being tested, compared with 20% of White men and 13% of Asian men, in the analysis of a large primary care cohort in the United Kingdom.
Incidence of advanced prostate cancer for Asian men with a raised PSA result was 4.5%, compared with 7.5% for White men and 7.0% for Black men.
Men included in the study were aged 40 and older and had no prior cancer diagnosis. Their ethnicity and PSA test result were logged in a national dataset between 2010 and 2017.
The study of more than 730,000 men, published in BMC Medicine, didn’t explore reasons for the differences, but experts offer their thoughts on what led to the findings and what these results imply.
Why the Higher Diagnosis Rates but Not More Advanced Disease in Black Men?
Lead author Liz Down, a graduate research assistant at the University of Exeter, Exeter, England, suggests the higher diagnosis rates but not more advanced disease in Black men may be linked to genetic variations.
Her team’s studies have shown that Black men in the United Kingdom and United States have higher levels of PSA. The PSA value is used to identify patients who might benefit from specialist investigation, and current guidelines in the UK and US don’t distinguish between ethnic groups.
As most men have slow-growing prostate cancer, this may lead to a disproportionately higher number of Black men being diagnosed with prostate cancer, she said.
“One possible interpretation,” Ms. Down notes, “is that prostate cancer follows a similar trajectory in Black and White men. What is different, however, is that Black men have higher PSA levels.”
As to why the advanced-cancer incidence is similar in Black and White patients in the study, Daniel George, MD, director of genitourinary oncology at Duke Cancer Institute in Durham, North Carolina, says it’s important to understand that the Black men in this study “are not necessarily representative of the Black population at large.”
In this study, “they’re a little bit more healthcare inclined,” Dr. George notes. The study population is actively seeking the PSA test. Their socioeconomic profile might be closer to their White counterparts’, and that may make results more similar, he said.
“It’s possible that because this is a screening and not just men coming in for symptoms or cause, that we’re not seeing as much advanced disease,” he continued.
Amar Kishan, MD, chief of the genitourinary oncology service at University of California Los Angeles (UCLA) Health, says the genomic factors and environmental stressors that lead to elevated PSA counts don’t necessarily translate into aggressiveness of disease.
Why do Different Races have Different Prostate Cancer Risk?
Dr. George points out that the study also highlights that Asian men were significantly less likely to be diagnosed with prostate cancer within 1 year of the test.
The reasons for differences in prostate risk by race are complex, he notes. There are some clues that biologic factors may be at work. For instance, early puberty has a link to prostate cancer as it does to breast cancer, and height is also associated with a greater risk of prostate cancer, Dr. George said.
It’s not necessarily a racial association but there are some biological factors associated with prostate cancer later in life, he explained. “These may be enriched in certain populations, including northern Europeans and patients with African ancestries.”
The study also notes that Black men are more likely to die from prostate cancer than are White men, and Asian men are less likely than White or Black men to die from it.
Ms. Down said the difference in prostate cancer mortality between Black vs White men, in particular, may be related to a number of factors, and age, and lifetime risk of prostate cancer may play a major role, at least in the UK.
Should There Be Different ‘Normal’ PSA Levels for Different Races?
Dr. George says there is likely a need to change the system because a PSA level in one race may not signal the same risk it does in another. So medicine probably needs to standardize what a “normal” PSA is by race, he says, adding that he is a coauthor of an upcoming paper regarding that issue.
The lowest instances of prostate cancer were in Asian patients so this isn’t just a Black and White issue, Dr. George notes. “Being able to establish benchmarks by race and ethnicity is something that is probably needed in the field,” he says.
Dr. Kishan, on the other hand, says data from this study are not enough to support differentiating PSA levels based on race. He noted a limitation of the study is that it was not able to calculate the false-negative rate of PSA tests.
What are the Implications for Treating and Screening for Prostate Cancer
Dr. Kishan says there may be a role for increased intensity of screening, whether at an earlier age or with different intervals, but prostate cancer treatment should not differ by race.
“Our prior study, as well as others,” he says, “have shown that when you balance Black and White patients for every factor that might impact prognosis other than race — such as age, disease aggressiveness, etc. — Black men actually tend to have better outcomes than White men. Thus, it would mean potentially overtreating (i.e., causing unnecessary side effects) to increase treatment intensity purely based on race with the available data.”
According to the paper, prostate cancer incidence in men with higher PSA levels increases with increasing age, even when using age-adjusted thresholds.
Dr. George says we know from this study and other studies as well that Black men are more likely to be diagnosed with prostate at a younger age. “Therefore, we probably need to be thinking about screening Black men starting at a younger age. These are the men who are most likely to benefit from an intervention — patients who have life expectancies of 20 years or more.”
What are the Downsides to Overdiagnosing Prostate Cancer in Men?
“It’s one of the biggest concerns that men have in proactively seeking healthcare,” Dr. George says. “They’re more likely to undergo treatment for this disease if they’re getting screened because (clinicians are) more likely to find it.”
Some of those men, he says, are going to undergo treatment for disease that won’t ultimately kill them, but may cause complications the men shouldn’t have had at all or otherwise may have had later.
“Overtreatment is a real concern. That’s why active surveillance is so important to minimize overtreatment of patients by finding out which cancers are low risk for progression and which are becoming more aggressive,” Dr. George says.
Authors of the study write that “the potential for overdiagnosis and the subsequent psychological and physical impact of diagnosis and treatment is an important consideration.”
All authors of the new paper received financial support from Cancer Research UK, the National Institute for Health and Care Research (NIHR), and the Higgins family for the submitted work.
Dr. George reports no relevant financial relationships.
Dr. Kishan reports consulting fees and speaking honoraria from Varian Medical Systems, Janssen, and Boston Scientific; research funding from PointBioPharma, Lantheus, and Janssen; and serving on advisory boards for Lantheus, Janssen and Boston Scientific.
FROM BMC MEDICINE
Outside the Guidelines: Denosumab Overuse in Prostate Cancer
Bone-modifying agents — most notably denosumab — are often prescribed to prevent skeletal-related complications in patients with metastatic castration-sensitive prostate cancer, but the drugs are not recommended for this indication and can lead to severe toxicities.
How much does Medicare spend each year on non-recommended bone therapy?
The answer, according to a new analysis in JCO Oncology Practice, is more than $44 million, with about $43 million coming from denosumab alone.
Overall, this study found that “the Medicare program pays tens of millions of dollars each year” for bone-modifying agents in patients with metastatic castration-sensitive prostate cancer, “which is not effective and may cause side effects,” lead author Aaron Mitchell, MD, MPH, a medical oncologist at Memorial Sloan Kettering Cancer Center, New York City, and colleagues concluded.
“These findings suggest reducing bone agent overuse could be a rare healthcare ‘win-win.’ Lower costs AND improved patient outcomes,” tweeted Dr. Mitchell. “If I were a payer, I’d be paying attention!”
In Prostate Cancer, Bone-Modifying Drug Indications Vary
Bone-modifying drugs are indicated for some patients with prostate cancer.
The American Society of Clinical Oncology has endorsed guidelines that recommend the use of denosumab in men with nonmetastatic prostate cancer at high risk for fracture while taking androgen deprivation therapy.
Among men with metastatic castration-resistant prostate cancer, guidelines also recommend zoledronic acid or denosumab for preventing or delaying skeletal-related events, such as pathologic fractures and spinal cord compression.
For patients with metastatic castration-sensitive disease, however, the bone-modifying agents show no benefit in preventing skeletal-related events and are not recommended for that indication.
In this population, “treatment with bone agents results only in avoidable toxicity and financial cost,” Dr. Mitchell tweeted. In its higher-dose formulation, denosumab comes with a price tag of approximately $40,000 per year in the United States.
An earlier study from Dr. Mitchell and colleagues revealed that the use of bone-modifying drugs to prevent skeletal events in metastatic castration-sensitive prostate cancer is common.
To better understand the costs associated with this inappropriate use, the researchers reviewed Surveillance, Epidemiology, and End Results Program Medicare data from 2011 to 2015. The team identified the frequency and number of doses of zoledronic acid and denosumab prescribed against recommendations in the metastatic castration-sensitive setting, making sure to distinguish between the use of denosumab to prevent osteoporotic fractures (appropriate use) and to prevent skeletal-related events (non-recommended use).
The team found that, among 2627 patients with metastatic castration-sensitive prostate cancer, 42% received at least one dose of denosumab and 18% received at least one dose of zoledronic acid.
The authors also found that unnecessary use of these drugs increased over time — with a little over 17% of patients receiving zoledronic acid between 2007 and 2009 and just over 28% receiving either denosumab (20.3%) or zoledronic acid (8.4%) from 2012 to 2015.
The annual costs to Medicare from non-recommended prescribing came to $44,105,041 for both agents, with the costs associated with denosumab representing the lion’s share at $43,303,078.
Non-recommended use of these agents also came with adverse events, such as femur fracture and hypocalcemia, which cost an estimated $758,450 to treat annually — $682,865 for denosumab and $75,585 for zoledronic acid.
The study focused on the Medicare-age population, which means the estimates are conservative. “Denosumab overuse for younger patients with castration-sensitive prostate cancer would add substantially to this total,” the authors wrote.
“This study contributes new evidence of overuse in the metastatic castrate-sensitive prostate cancer setting, which I must admit reflects my clinical experience in seeing patients for second opinions who are treated in the community,” said Samuel U. Takvorian, MD, of the Division of Hematology and Oncology, Perelman School of Medicine, Philadelphia, who wasn’t involved in the research. “While there are some circumstances in which one would consider using a bone-modifying agent in the metastatic castrate-sensitive prostate cancer setting, most [of these] men don’t need them upfront.”
Why Is the Overuse Happening?
One reason for the inappropriate use of bone-modifying drugs could be confusion surrounding the recommendations because the drugs are recommended for some patients with prostate cancer.
Michael R. Laurent, MD, PhD, of Imelda Hospital, Bonheiden, Belgium, explained that the use of bone-modifying drugs is, paradoxically, often overlooked in settings where they are recommended — when patients have an elevated risk for osteoporosis or fracture.
“Guidelines are quite unequivocal in their recommendations to prevent osteoporosis in mostly older men who receive androgen deprivation therapy,” but “I think there is significant undertreatment” in these patients, Dr. Laurent told this news organization.
However, the recommendation for patients at risk for osteoporosis or bone fracture calls for less intense regimens, which may include lower-dose denosumab, administered once every 6 months, zoledronic acid, given yearly, or another lower potency agent, such as oral alendronate weekly, explained Philip J. Saylor, MD, an attending physician at Massachusetts General Hospital and assistant professor at Harvard Medical School, Boston.
Meanwhile, “monthly high-intensity therapy to prevent skeletal events should be reserved specifically for bone metastatic castration-resistant prostate cancer for more than just cost reasons,” Dr. Saylor said.
When it comes to the higher dose, monthly therapy in castration-sensitive prostate cancer, “we have no evidence that it is beneficial,” he said, adding that “when the prostate cancer itself is well controlled by hormonal therapy, there just aren’t very many pathologic fractures or other bone complications.”
Alongside possible confusion over the recommendations, many physicians also likely don’t know how much denosumab costs.
“In our recent physician interview study, we did find that most physicians were very much unaware of the cost of this drug, or the cost difference between denosumab and zoledronic acid, so I do think that lack of cost awareness is a factor,” Dr. Mitchell said.
Part of the reason may be how Medicare covers these agents. Typically, Medicare would not cover non-recommended indications, but “in this case, Medicare coverage is broader and includes both the guideline-recommended and non-recommended uses,” Dr. Mitchell explained.
However, the authors also identified a more cynical reason for non-recommended prescribing — promotional payments from drug makers to physicians.
In another recent paper, Dr. Mitchell said he found about “30% of doctors treating prostate cancer had received payments from Amgen for Xgeva [denosumab] promotion during the last year.”
These payments appeared to influence non-recommended prescribing: Among patients whose doctor had not received payments, 31.4% received non-recommended denosumab, which increased to nearly 50% of patients among doctors who had received payments.
Dr. Mitchell suggested a few ways to help curb inappropriate prescribing.
Medicare could, for instance, change its coverage policy to include only the recommended uses of these agents, Dr. Mitchell said.
More physician education would be another solution. “I think that physician education would be one ‘bottom-up’ approach that could work,” Dr. Mitchell added.
Dr. Mitchell, Dr. Takvorian, and Dr. Saylor had no disclosures to report. Dr. Laurent has received lecture and consultancy fees from Alexion, AM Pharma, Amgen, Galapagos, Kyowa Kirin, Menarini, Orifarm, Pharmanovia, Takeda, UCB, and Will Pharma.
A version of this article appeared on Medscape.com.
Bone-modifying agents — most notably denosumab — are often prescribed to prevent skeletal-related complications in patients with metastatic castration-sensitive prostate cancer, but the drugs are not recommended for this indication and can lead to severe toxicities.
How much does Medicare spend each year on non-recommended bone therapy?
The answer, according to a new analysis in JCO Oncology Practice, is more than $44 million, with about $43 million coming from denosumab alone.
Overall, this study found that “the Medicare program pays tens of millions of dollars each year” for bone-modifying agents in patients with metastatic castration-sensitive prostate cancer, “which is not effective and may cause side effects,” lead author Aaron Mitchell, MD, MPH, a medical oncologist at Memorial Sloan Kettering Cancer Center, New York City, and colleagues concluded.
“These findings suggest reducing bone agent overuse could be a rare healthcare ‘win-win.’ Lower costs AND improved patient outcomes,” tweeted Dr. Mitchell. “If I were a payer, I’d be paying attention!”
In Prostate Cancer, Bone-Modifying Drug Indications Vary
Bone-modifying drugs are indicated for some patients with prostate cancer.
The American Society of Clinical Oncology has endorsed guidelines that recommend the use of denosumab in men with nonmetastatic prostate cancer at high risk for fracture while taking androgen deprivation therapy.
Among men with metastatic castration-resistant prostate cancer, guidelines also recommend zoledronic acid or denosumab for preventing or delaying skeletal-related events, such as pathologic fractures and spinal cord compression.
For patients with metastatic castration-sensitive disease, however, the bone-modifying agents show no benefit in preventing skeletal-related events and are not recommended for that indication.
In this population, “treatment with bone agents results only in avoidable toxicity and financial cost,” Dr. Mitchell tweeted. In its higher-dose formulation, denosumab comes with a price tag of approximately $40,000 per year in the United States.
An earlier study from Dr. Mitchell and colleagues revealed that the use of bone-modifying drugs to prevent skeletal events in metastatic castration-sensitive prostate cancer is common.
To better understand the costs associated with this inappropriate use, the researchers reviewed Surveillance, Epidemiology, and End Results Program Medicare data from 2011 to 2015. The team identified the frequency and number of doses of zoledronic acid and denosumab prescribed against recommendations in the metastatic castration-sensitive setting, making sure to distinguish between the use of denosumab to prevent osteoporotic fractures (appropriate use) and to prevent skeletal-related events (non-recommended use).
The team found that, among 2627 patients with metastatic castration-sensitive prostate cancer, 42% received at least one dose of denosumab and 18% received at least one dose of zoledronic acid.
The authors also found that unnecessary use of these drugs increased over time — with a little over 17% of patients receiving zoledronic acid between 2007 and 2009 and just over 28% receiving either denosumab (20.3%) or zoledronic acid (8.4%) from 2012 to 2015.
The annual costs to Medicare from non-recommended prescribing came to $44,105,041 for both agents, with the costs associated with denosumab representing the lion’s share at $43,303,078.
Non-recommended use of these agents also came with adverse events, such as femur fracture and hypocalcemia, which cost an estimated $758,450 to treat annually — $682,865 for denosumab and $75,585 for zoledronic acid.
The study focused on the Medicare-age population, which means the estimates are conservative. “Denosumab overuse for younger patients with castration-sensitive prostate cancer would add substantially to this total,” the authors wrote.
“This study contributes new evidence of overuse in the metastatic castrate-sensitive prostate cancer setting, which I must admit reflects my clinical experience in seeing patients for second opinions who are treated in the community,” said Samuel U. Takvorian, MD, of the Division of Hematology and Oncology, Perelman School of Medicine, Philadelphia, who wasn’t involved in the research. “While there are some circumstances in which one would consider using a bone-modifying agent in the metastatic castrate-sensitive prostate cancer setting, most [of these] men don’t need them upfront.”
Why Is the Overuse Happening?
One reason for the inappropriate use of bone-modifying drugs could be confusion surrounding the recommendations because the drugs are recommended for some patients with prostate cancer.
Michael R. Laurent, MD, PhD, of Imelda Hospital, Bonheiden, Belgium, explained that the use of bone-modifying drugs is, paradoxically, often overlooked in settings where they are recommended — when patients have an elevated risk for osteoporosis or fracture.
“Guidelines are quite unequivocal in their recommendations to prevent osteoporosis in mostly older men who receive androgen deprivation therapy,” but “I think there is significant undertreatment” in these patients, Dr. Laurent told this news organization.
However, the recommendation for patients at risk for osteoporosis or bone fracture calls for less intense regimens, which may include lower-dose denosumab, administered once every 6 months, zoledronic acid, given yearly, or another lower potency agent, such as oral alendronate weekly, explained Philip J. Saylor, MD, an attending physician at Massachusetts General Hospital and assistant professor at Harvard Medical School, Boston.
Meanwhile, “monthly high-intensity therapy to prevent skeletal events should be reserved specifically for bone metastatic castration-resistant prostate cancer for more than just cost reasons,” Dr. Saylor said.
When it comes to the higher dose, monthly therapy in castration-sensitive prostate cancer, “we have no evidence that it is beneficial,” he said, adding that “when the prostate cancer itself is well controlled by hormonal therapy, there just aren’t very many pathologic fractures or other bone complications.”
Alongside possible confusion over the recommendations, many physicians also likely don’t know how much denosumab costs.
“In our recent physician interview study, we did find that most physicians were very much unaware of the cost of this drug, or the cost difference between denosumab and zoledronic acid, so I do think that lack of cost awareness is a factor,” Dr. Mitchell said.
Part of the reason may be how Medicare covers these agents. Typically, Medicare would not cover non-recommended indications, but “in this case, Medicare coverage is broader and includes both the guideline-recommended and non-recommended uses,” Dr. Mitchell explained.
However, the authors also identified a more cynical reason for non-recommended prescribing — promotional payments from drug makers to physicians.
In another recent paper, Dr. Mitchell said he found about “30% of doctors treating prostate cancer had received payments from Amgen for Xgeva [denosumab] promotion during the last year.”
These payments appeared to influence non-recommended prescribing: Among patients whose doctor had not received payments, 31.4% received non-recommended denosumab, which increased to nearly 50% of patients among doctors who had received payments.
Dr. Mitchell suggested a few ways to help curb inappropriate prescribing.
Medicare could, for instance, change its coverage policy to include only the recommended uses of these agents, Dr. Mitchell said.
More physician education would be another solution. “I think that physician education would be one ‘bottom-up’ approach that could work,” Dr. Mitchell added.
Dr. Mitchell, Dr. Takvorian, and Dr. Saylor had no disclosures to report. Dr. Laurent has received lecture and consultancy fees from Alexion, AM Pharma, Amgen, Galapagos, Kyowa Kirin, Menarini, Orifarm, Pharmanovia, Takeda, UCB, and Will Pharma.
A version of this article appeared on Medscape.com.
Bone-modifying agents — most notably denosumab — are often prescribed to prevent skeletal-related complications in patients with metastatic castration-sensitive prostate cancer, but the drugs are not recommended for this indication and can lead to severe toxicities.
How much does Medicare spend each year on non-recommended bone therapy?
The answer, according to a new analysis in JCO Oncology Practice, is more than $44 million, with about $43 million coming from denosumab alone.
Overall, this study found that “the Medicare program pays tens of millions of dollars each year” for bone-modifying agents in patients with metastatic castration-sensitive prostate cancer, “which is not effective and may cause side effects,” lead author Aaron Mitchell, MD, MPH, a medical oncologist at Memorial Sloan Kettering Cancer Center, New York City, and colleagues concluded.
“These findings suggest reducing bone agent overuse could be a rare healthcare ‘win-win.’ Lower costs AND improved patient outcomes,” tweeted Dr. Mitchell. “If I were a payer, I’d be paying attention!”
In Prostate Cancer, Bone-Modifying Drug Indications Vary
Bone-modifying drugs are indicated for some patients with prostate cancer.
The American Society of Clinical Oncology has endorsed guidelines that recommend the use of denosumab in men with nonmetastatic prostate cancer at high risk for fracture while taking androgen deprivation therapy.
Among men with metastatic castration-resistant prostate cancer, guidelines also recommend zoledronic acid or denosumab for preventing or delaying skeletal-related events, such as pathologic fractures and spinal cord compression.
For patients with metastatic castration-sensitive disease, however, the bone-modifying agents show no benefit in preventing skeletal-related events and are not recommended for that indication.
In this population, “treatment with bone agents results only in avoidable toxicity and financial cost,” Dr. Mitchell tweeted. In its higher-dose formulation, denosumab comes with a price tag of approximately $40,000 per year in the United States.
An earlier study from Dr. Mitchell and colleagues revealed that the use of bone-modifying drugs to prevent skeletal events in metastatic castration-sensitive prostate cancer is common.
To better understand the costs associated with this inappropriate use, the researchers reviewed Surveillance, Epidemiology, and End Results Program Medicare data from 2011 to 2015. The team identified the frequency and number of doses of zoledronic acid and denosumab prescribed against recommendations in the metastatic castration-sensitive setting, making sure to distinguish between the use of denosumab to prevent osteoporotic fractures (appropriate use) and to prevent skeletal-related events (non-recommended use).
The team found that, among 2627 patients with metastatic castration-sensitive prostate cancer, 42% received at least one dose of denosumab and 18% received at least one dose of zoledronic acid.
The authors also found that unnecessary use of these drugs increased over time — with a little over 17% of patients receiving zoledronic acid between 2007 and 2009 and just over 28% receiving either denosumab (20.3%) or zoledronic acid (8.4%) from 2012 to 2015.
The annual costs to Medicare from non-recommended prescribing came to $44,105,041 for both agents, with the costs associated with denosumab representing the lion’s share at $43,303,078.
Non-recommended use of these agents also came with adverse events, such as femur fracture and hypocalcemia, which cost an estimated $758,450 to treat annually — $682,865 for denosumab and $75,585 for zoledronic acid.
The study focused on the Medicare-age population, which means the estimates are conservative. “Denosumab overuse for younger patients with castration-sensitive prostate cancer would add substantially to this total,” the authors wrote.
“This study contributes new evidence of overuse in the metastatic castrate-sensitive prostate cancer setting, which I must admit reflects my clinical experience in seeing patients for second opinions who are treated in the community,” said Samuel U. Takvorian, MD, of the Division of Hematology and Oncology, Perelman School of Medicine, Philadelphia, who wasn’t involved in the research. “While there are some circumstances in which one would consider using a bone-modifying agent in the metastatic castrate-sensitive prostate cancer setting, most [of these] men don’t need them upfront.”
Why Is the Overuse Happening?
One reason for the inappropriate use of bone-modifying drugs could be confusion surrounding the recommendations because the drugs are recommended for some patients with prostate cancer.
Michael R. Laurent, MD, PhD, of Imelda Hospital, Bonheiden, Belgium, explained that the use of bone-modifying drugs is, paradoxically, often overlooked in settings where they are recommended — when patients have an elevated risk for osteoporosis or fracture.
“Guidelines are quite unequivocal in their recommendations to prevent osteoporosis in mostly older men who receive androgen deprivation therapy,” but “I think there is significant undertreatment” in these patients, Dr. Laurent told this news organization.
However, the recommendation for patients at risk for osteoporosis or bone fracture calls for less intense regimens, which may include lower-dose denosumab, administered once every 6 months, zoledronic acid, given yearly, or another lower potency agent, such as oral alendronate weekly, explained Philip J. Saylor, MD, an attending physician at Massachusetts General Hospital and assistant professor at Harvard Medical School, Boston.
Meanwhile, “monthly high-intensity therapy to prevent skeletal events should be reserved specifically for bone metastatic castration-resistant prostate cancer for more than just cost reasons,” Dr. Saylor said.
When it comes to the higher dose, monthly therapy in castration-sensitive prostate cancer, “we have no evidence that it is beneficial,” he said, adding that “when the prostate cancer itself is well controlled by hormonal therapy, there just aren’t very many pathologic fractures or other bone complications.”
Alongside possible confusion over the recommendations, many physicians also likely don’t know how much denosumab costs.
“In our recent physician interview study, we did find that most physicians were very much unaware of the cost of this drug, or the cost difference between denosumab and zoledronic acid, so I do think that lack of cost awareness is a factor,” Dr. Mitchell said.
Part of the reason may be how Medicare covers these agents. Typically, Medicare would not cover non-recommended indications, but “in this case, Medicare coverage is broader and includes both the guideline-recommended and non-recommended uses,” Dr. Mitchell explained.
However, the authors also identified a more cynical reason for non-recommended prescribing — promotional payments from drug makers to physicians.
In another recent paper, Dr. Mitchell said he found about “30% of doctors treating prostate cancer had received payments from Amgen for Xgeva [denosumab] promotion during the last year.”
These payments appeared to influence non-recommended prescribing: Among patients whose doctor had not received payments, 31.4% received non-recommended denosumab, which increased to nearly 50% of patients among doctors who had received payments.
Dr. Mitchell suggested a few ways to help curb inappropriate prescribing.
Medicare could, for instance, change its coverage policy to include only the recommended uses of these agents, Dr. Mitchell said.
More physician education would be another solution. “I think that physician education would be one ‘bottom-up’ approach that could work,” Dr. Mitchell added.
Dr. Mitchell, Dr. Takvorian, and Dr. Saylor had no disclosures to report. Dr. Laurent has received lecture and consultancy fees from Alexion, AM Pharma, Amgen, Galapagos, Kyowa Kirin, Menarini, Orifarm, Pharmanovia, Takeda, UCB, and Will Pharma.
A version of this article appeared on Medscape.com.
Is MRI Screening Unnecessarily High in Prostate Cancer?
TOPLINE:
METHODOLOGY:
- New initiatives are focusing on organizing prostate cancer screening using MRI to reduce overdiagnosis, as current evidence does not support the effectiveness of a single PSA test, with guidelines now recommending repeated testing every 1-4 years.
- In the STHLM3-MRI trial, men, aged 50-74 years, living in Stockholm County, Sweden, were invited to participate in prostate cancer screening and randomly assigned to traditional screening with systematic or an MRI-based strategy.
- Blood samples were analyzed for PSA levels and Stockholm3 risk score; men with elevated risk underwent targeted MRI and biopsy procedures.
- In this follow-up analysis, 2,078 men with PSA levels of 1.5 ng/mL or higher and a Stockholm3 risk score less than 0.11 were re-invited for screening 2-3 years after their initial screening.
- The primary outcome was clinically significant prostate cancer (Gleason score of 3 + 4 or greater). A Gleason score of 6 was detected in 0.7% of patients, and a score of 4 + 3 or greater was detected in 19 (1.3%) men.
TAKEAWAY:
- Of 1,500 men (median age of 67 years) who underwent a blood test, the median PSA level was 2.8 ng/mL and 26.0% changed risk classification groups (PSA levels < 3 vs 3 ng/mL).
- Out of 667 men with PSA levels of 3 ng/mL or higher, 617 (92.5%) had an MRI. Of the 617, 51 (7.6%) had equivocal lesions (a Prostate Imaging-Reporting and Data System score of 3) and 33 (4.9%) had suspicious lesions.
- Of the 1,500 rescreened men, clinically significant prostate cancer was detected in 48 men (3.2%); this corresponds to 59.2% of the biopsied men.
- Out of 383 men who had previously received a negative MRI result, only 10 (2.6%) exhibited a lesion with a Prostate Imaging-Reporting and Data System score of 4 or higher.
IN PRACTICE:
In an accompanying editorial, Ola Bratt, MD, PhD, noted that the “most important finding was the very high proportion of nonsuspicious repeat MRI scans,” but also emphasizes the necessity of observing a decrease in overall prostate cancer incidence before asserting that the current cancer diagnostics effectively reduce overdiagnosis.
SOURCE:
This study, led by Tobias Nordström, MD, PhD, from Karolinska Institute, Stockholm, Sweden, was published on February 7, 2024, in JAMA Network Open.
LIMITATIONS:
Long-term outcomes like prostate cancer mortality were not evaluated. Information on cancer detection in men with a negative MRI result at rescreening was not available. Authors noted that a subset of individuals may still be at risk despite lower PSA levels.
DISCLOSURES:
This study was funded by the Swedish Research Council for Health, Working Life and Welfare, Karolinska Institute, Prostatacancerförbundet, Region Stockholm, and Åke Wibergs Stiftelse. The authors reported financial relationships outside this work.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- New initiatives are focusing on organizing prostate cancer screening using MRI to reduce overdiagnosis, as current evidence does not support the effectiveness of a single PSA test, with guidelines now recommending repeated testing every 1-4 years.
- In the STHLM3-MRI trial, men, aged 50-74 years, living in Stockholm County, Sweden, were invited to participate in prostate cancer screening and randomly assigned to traditional screening with systematic or an MRI-based strategy.
- Blood samples were analyzed for PSA levels and Stockholm3 risk score; men with elevated risk underwent targeted MRI and biopsy procedures.
- In this follow-up analysis, 2,078 men with PSA levels of 1.5 ng/mL or higher and a Stockholm3 risk score less than 0.11 were re-invited for screening 2-3 years after their initial screening.
- The primary outcome was clinically significant prostate cancer (Gleason score of 3 + 4 or greater). A Gleason score of 6 was detected in 0.7% of patients, and a score of 4 + 3 or greater was detected in 19 (1.3%) men.
TAKEAWAY:
- Of 1,500 men (median age of 67 years) who underwent a blood test, the median PSA level was 2.8 ng/mL and 26.0% changed risk classification groups (PSA levels < 3 vs 3 ng/mL).
- Out of 667 men with PSA levels of 3 ng/mL or higher, 617 (92.5%) had an MRI. Of the 617, 51 (7.6%) had equivocal lesions (a Prostate Imaging-Reporting and Data System score of 3) and 33 (4.9%) had suspicious lesions.
- Of the 1,500 rescreened men, clinically significant prostate cancer was detected in 48 men (3.2%); this corresponds to 59.2% of the biopsied men.
- Out of 383 men who had previously received a negative MRI result, only 10 (2.6%) exhibited a lesion with a Prostate Imaging-Reporting and Data System score of 4 or higher.
IN PRACTICE:
In an accompanying editorial, Ola Bratt, MD, PhD, noted that the “most important finding was the very high proportion of nonsuspicious repeat MRI scans,” but also emphasizes the necessity of observing a decrease in overall prostate cancer incidence before asserting that the current cancer diagnostics effectively reduce overdiagnosis.
SOURCE:
This study, led by Tobias Nordström, MD, PhD, from Karolinska Institute, Stockholm, Sweden, was published on February 7, 2024, in JAMA Network Open.
LIMITATIONS:
Long-term outcomes like prostate cancer mortality were not evaluated. Information on cancer detection in men with a negative MRI result at rescreening was not available. Authors noted that a subset of individuals may still be at risk despite lower PSA levels.
DISCLOSURES:
This study was funded by the Swedish Research Council for Health, Working Life and Welfare, Karolinska Institute, Prostatacancerförbundet, Region Stockholm, and Åke Wibergs Stiftelse. The authors reported financial relationships outside this work.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- New initiatives are focusing on organizing prostate cancer screening using MRI to reduce overdiagnosis, as current evidence does not support the effectiveness of a single PSA test, with guidelines now recommending repeated testing every 1-4 years.
- In the STHLM3-MRI trial, men, aged 50-74 years, living in Stockholm County, Sweden, were invited to participate in prostate cancer screening and randomly assigned to traditional screening with systematic or an MRI-based strategy.
- Blood samples were analyzed for PSA levels and Stockholm3 risk score; men with elevated risk underwent targeted MRI and biopsy procedures.
- In this follow-up analysis, 2,078 men with PSA levels of 1.5 ng/mL or higher and a Stockholm3 risk score less than 0.11 were re-invited for screening 2-3 years after their initial screening.
- The primary outcome was clinically significant prostate cancer (Gleason score of 3 + 4 or greater). A Gleason score of 6 was detected in 0.7% of patients, and a score of 4 + 3 or greater was detected in 19 (1.3%) men.
TAKEAWAY:
- Of 1,500 men (median age of 67 years) who underwent a blood test, the median PSA level was 2.8 ng/mL and 26.0% changed risk classification groups (PSA levels < 3 vs 3 ng/mL).
- Out of 667 men with PSA levels of 3 ng/mL or higher, 617 (92.5%) had an MRI. Of the 617, 51 (7.6%) had equivocal lesions (a Prostate Imaging-Reporting and Data System score of 3) and 33 (4.9%) had suspicious lesions.
- Of the 1,500 rescreened men, clinically significant prostate cancer was detected in 48 men (3.2%); this corresponds to 59.2% of the biopsied men.
- Out of 383 men who had previously received a negative MRI result, only 10 (2.6%) exhibited a lesion with a Prostate Imaging-Reporting and Data System score of 4 or higher.
IN PRACTICE:
In an accompanying editorial, Ola Bratt, MD, PhD, noted that the “most important finding was the very high proportion of nonsuspicious repeat MRI scans,” but also emphasizes the necessity of observing a decrease in overall prostate cancer incidence before asserting that the current cancer diagnostics effectively reduce overdiagnosis.
SOURCE:
This study, led by Tobias Nordström, MD, PhD, from Karolinska Institute, Stockholm, Sweden, was published on February 7, 2024, in JAMA Network Open.
LIMITATIONS:
Long-term outcomes like prostate cancer mortality were not evaluated. Information on cancer detection in men with a negative MRI result at rescreening was not available. Authors noted that a subset of individuals may still be at risk despite lower PSA levels.
DISCLOSURES:
This study was funded by the Swedish Research Council for Health, Working Life and Welfare, Karolinska Institute, Prostatacancerförbundet, Region Stockholm, and Åke Wibergs Stiftelse. The authors reported financial relationships outside this work.
A version of this article appeared on Medscape.com.
Focal Therapy for Prostate Cancer: Evidence-Based or Oversold?
In 2013, a prostate-specific antigen (PSA) blood test revealed that Richard LaFrate’s levels had jumped.
Previously in a normal range, his PSA was now above 6 ng/mL, indicating an elevated likelihood for prostate cancer. The jazz guitarist from Leesburg, Florida, then 70 years old, underwent a biopsy, which found two Gleason 6 lesions.
Mr. LaFrate had low-risk prostate cancer.
Guidelines now recommend active surveillance for patients like Mr. LaFrate, who have low-risk disease. This strategy would mean monitoring the cancer until LaFrate required treatment, with the upside being he might never need therapy.
Mr. LaFrate’s urologist, however, was pushing whole gland surgery — an invasive and unnecessary procedure given his diagnosis and age.
Mr. LaFrate decided to look for another doctor. He filled out a form online that pointed him to a new urologist who offered him one option: An investigational procedure known as high-intensity focused ultrasound.
At the time, high-intensity focused ultrasound — a form of focal therapy — was being studied in the United States to treat men with low or intermediate-risk prostate cancer, but it was still relatively early days.
Mr. LaFrate’s urologist asked him to pay $25,000 out of pocket to undergo the focal procedure at a clinic in the Bahamas. He refused and, ultimately, landed on active surveillance as the best strategy to manage for his low-risk disease.
That urologist was “a shyster in my opinion,” Mr. LaFrate said.
— Gleason 3+4 (grade group 2) tumors — as an alternative to invasive surgery and active surveillance. Prestigious medical centers, such as Cleveland Clinic, Mayo Clinic, Memorial Sloan Kettering, UCLA, and the University of Chicago, routinely offer focal therapy.
But use of the techniques remains controversial and costly.
As the Cleveland Clinic’s website acknowledges, although “the use of focal therapy for localized prostate cancer appears to be a promising development in a number of ways, it is still considered investigational and not yet part of standard therapy.” Major caveats to focal therapy include unknown long-term effectiveness, the possibility of leaving behind untreated cancer, and higher overall costs.
No major national guidelines endorse the use of focal therapy, unless offered in a research or clinical trial setting. Insurance companies, such as Aetna, Blue Cross Blue Shield, and United, also consider focal therapy for prostate cancer investigational and don’t cover it.
Without a stamp of approval from guideline bodies and insurance companies, patients, like Mr. LaFrate, remain vulnerable to the high out-of-pocket costs for these focal techniques.
“Almost every place charges $15,000-$30,000 in cash,” said Daniel Spratt, MD, radiation oncology chair at University Hospitals Seidman Cancer Center and Case Western Reserve University in Cleveland.
Dr. Spratt has seen hundreds of patients after focal therapy, some from prominent centers, who have emptied their bank accounts to undergo treatment with the promise of great results and ultimately felt misled when the cancer has recurred.
“It pains me that there are doctors willing to ignore the Hippocratic oath of ‘Do No Harm’ simply to jump on this fad to bring in revenue,” Dr. Spratt said.
Evidence-Based or Oversold?
Focal therapy gained a foothold in the United Kingdom well before the United States.
Hashim Ahmed, FRCS, urology chair at Imperial College London, has used focal therapy for 15 years, treated over 1000 patients, and taught dozens of surgeons how to use the leading focal therapies — focal cryoablation, in which surgeons use a needle-thin probe to target, freeze, and kill prostate tumors, as well as high-intensity focused ultrasound, which uses sound wave energy to superheat and kill tumors.
“Certainly, in the United Kingdom, focal therapy has been prime time in a number of centers for a number of years,” Dr. Ahmed said.
In the United States, focal therapy has become an attractive option for men with prostate cancer who want to avoid radiation or radical prostatectomy but don’t feel comfortable simply monitoring their disease with active surveillance. Experts from specialized focal therapy centers touting the promise of this “innovative technique” predict its routine use in the next few years.
But the excitement surrounding the use of focal therapy in prostate cancer has outpaced broader acceptance.
In 2015, the FDA approved high-intensity focused ultrasound to treat prostatic disease, but not prostate cancer specifically. Although the approval language “means that companies cannot advertise that their devices can be used for prostate cancer,” physicians can still determine how to use the technology, which includes treating prostate cancer, Dr. Ahmed said.
The evidence is starting to catch up to the demand. The latest research suggests that the partial-gland techniques may stand up well to radical prostatectomy.
A 2022 prospective database study comparing radical prostatectomies to focal therapy — mostly high-intensity focused ultrasound — in more than 800 men found similar rates of failure-free survival in the two groups at the 8-year follow-up. A 2019 registry study found that failure-free survival at 3 years was just over 90% in high and intermediate-risk patients receiving focal cryotherapy, with the rate rising to about 93% for the intermediate-risk group. And a 2018 prospective study of 625 patients with intermediate or high-risk prostate cancer who underwent high-intensity focused ultrasound had 5-year metastasis-free survival of 98% and overall survival rates of 100%.
One of the biggest draws of focal therapy vs more aggressive treatments is the “massive differences in side-effect profiles,” said Dr. Ahmed.
In a 2021 meta-analysis, researchers found that 6 months after high-intensity focused ultrasound, 98% of patients remained continent and 80% retained erectile function, while erectile dysfunction can occur in 30% to as many as 85% of patients following prostatectomy or radiotherapy and urinary incontinence can occur in as many as 40% of patients.
Despite these potential advantages of focal therapy, the long-term efficacy of the techniques remains uncertain.
A recent study from a team at MSK, for instance, reported that 40% of men with intermediate (grade 2) or high-risk (grade 3) disease had residual cancer following MRI-guided focused ultrasound. A 2020 prospective registry study found that almost 20% of patients undergoing high-intensity focal ultrasound required a second round following a recurrence.
Dr. Spratt worries that patients who recur after focal therapy may go on to receive a second round — often offered at half price — and will still ultimately need surgery or radiation therapy later. By that point, however, patients may have spent as much as $45,000 — ie, $30,000 on the initial and another $15,000 on the follow-up procedure.
When patients see Dr. Spratt after a recurrence, he informs them that their side effects will be worse if he gives them radiation or surgery now vs if he had given them curative therapy upfront. “But this is what we’re left with,” he tells them.
Another big concern in the field is “the quality of data for focal therapy is overwhelmingly poor,” said Jonathan Shoag, MD, a urologic oncologist at University Hospitals and an associate professor of urology at Case Western Reserve University School of Medicine in Cleveland. “Essentially, the bulk of the data is from single-institution retrospective series without defined follow-up protocols or endpoints.”
The American Urological Association (AUA) has even cautioned experts and patients about the lack of high-quality data comparing focal therapy techniques to radiation therapy, surgery, and active surveillance. According to the AUA, focal options should only be considered in intermediate-risk prostate cancer in a clinical trial setting.
“The lack of randomized clinical trials poses a major stumbling block for the field,” said Dr. Ahmed.
Although randomized trials would be ideal, the results would take many years to mature, and growing patient demand for these less invasive focal procedures has made randomized trials difficult to complete, explained Arvin George, MD, associate professor at Johns Hopkins School of Medicine in Baltimore. Several randomized trials attempted in Norway and the United Kingdom, for instance, fell apart when patients refused to be randomized between focal and radical therapy, Dr. George said.
Focal therapy is now in the same position that active surveillance was a few years ago, according to Dr. George.
“We are hearing the same concerns about focal therapy now as we did about active surveillance,” he said. The initial evidence supporting active surveillance largely came from real-world experience and retrospective studies. The randomized data came later, and skeptics of active surveillance “were proven wrong,” he added.
But Dr. Shoag has a different take on the trajectory of focal therapy research and care in the United States.
“I think there’s this emerging kind of tragedy happening in our field now, where you have even academic institutions offering focal therapy to patients off-trial with essentially no data to suggest it is oncologically effective,” Dr. Shoag said.
William Catalona, MD, Northwestern University Feinberg School of Medicine, Chicago, agreed, noting that too many low-risk patients are undergoing focal treatment who should be on active surveillance. “Many men are attracted to focal because they just are uncomfortable having a cancer in their body that’s not treated,” Dr. Catalona said. But “giving these patients focal therapy is really overtreatment.”
Patients with higher-risk disease who want to avoid aggressive treatment are also being lured into focal without guidelines or clear evidence to back up that option, Dr. Catalona explained.
Although it’s not clear how many men in the United States are receiving focal therapy who shouldn’t, even proponents of focal therapy, like George, have expressed concern.
Dr. George agreed that focal therapy marketing geared towards patients is drawing in some men who are not good candidates for these techniques, and feels there’s not enough objective material from medical societies or academic centers giving patients a realistic picture of focal therapy.
“There is concern that patients may be receiving biased information,” Dr. George said, adding that it’s ultimately up to the physician to reconcile the best available evidence, understand the outcomes, and discuss these options with the patient to guide them to what’s best.
At the end of the day, Dr. Spratt said, physicians giving focal therapy off a clinical trial need to pause and ask themselves “why are they giving a treatment that remains investigational by payers, not recommended by any major guideline, and that lacks any randomized evidence?”
Mr. LaFrate does not regret his decision to forgo focal therapy in 2013. He has been on active surveillance for about a decade now.
Following an MRI in 2022, Mr. LaFrate’s radiology report found that “clinically significant cancer is very unlikely to be present.”
Still, his PSA has risen two points in the past year to 14. His current urologist feels that the PSA is going up because there’s cancer present and is suggesting focal therapy for Mr. LaFrate.
Mr. LaFrate, who has prostate enlargement issues, remains skeptical of focal therapy and is still resisting the sales pitch.
“My doctor is not aggressively pushing it. He’s just giving me that as one of my options,” he said. “I just have a hunch I don’t need it at this point.”
A version of this article appeared on Medscape.com.
In 2013, a prostate-specific antigen (PSA) blood test revealed that Richard LaFrate’s levels had jumped.
Previously in a normal range, his PSA was now above 6 ng/mL, indicating an elevated likelihood for prostate cancer. The jazz guitarist from Leesburg, Florida, then 70 years old, underwent a biopsy, which found two Gleason 6 lesions.
Mr. LaFrate had low-risk prostate cancer.
Guidelines now recommend active surveillance for patients like Mr. LaFrate, who have low-risk disease. This strategy would mean monitoring the cancer until LaFrate required treatment, with the upside being he might never need therapy.
Mr. LaFrate’s urologist, however, was pushing whole gland surgery — an invasive and unnecessary procedure given his diagnosis and age.
Mr. LaFrate decided to look for another doctor. He filled out a form online that pointed him to a new urologist who offered him one option: An investigational procedure known as high-intensity focused ultrasound.
At the time, high-intensity focused ultrasound — a form of focal therapy — was being studied in the United States to treat men with low or intermediate-risk prostate cancer, but it was still relatively early days.
Mr. LaFrate’s urologist asked him to pay $25,000 out of pocket to undergo the focal procedure at a clinic in the Bahamas. He refused and, ultimately, landed on active surveillance as the best strategy to manage for his low-risk disease.
That urologist was “a shyster in my opinion,” Mr. LaFrate said.
— Gleason 3+4 (grade group 2) tumors — as an alternative to invasive surgery and active surveillance. Prestigious medical centers, such as Cleveland Clinic, Mayo Clinic, Memorial Sloan Kettering, UCLA, and the University of Chicago, routinely offer focal therapy.
But use of the techniques remains controversial and costly.
As the Cleveland Clinic’s website acknowledges, although “the use of focal therapy for localized prostate cancer appears to be a promising development in a number of ways, it is still considered investigational and not yet part of standard therapy.” Major caveats to focal therapy include unknown long-term effectiveness, the possibility of leaving behind untreated cancer, and higher overall costs.
No major national guidelines endorse the use of focal therapy, unless offered in a research or clinical trial setting. Insurance companies, such as Aetna, Blue Cross Blue Shield, and United, also consider focal therapy for prostate cancer investigational and don’t cover it.
Without a stamp of approval from guideline bodies and insurance companies, patients, like Mr. LaFrate, remain vulnerable to the high out-of-pocket costs for these focal techniques.
“Almost every place charges $15,000-$30,000 in cash,” said Daniel Spratt, MD, radiation oncology chair at University Hospitals Seidman Cancer Center and Case Western Reserve University in Cleveland.
Dr. Spratt has seen hundreds of patients after focal therapy, some from prominent centers, who have emptied their bank accounts to undergo treatment with the promise of great results and ultimately felt misled when the cancer has recurred.
“It pains me that there are doctors willing to ignore the Hippocratic oath of ‘Do No Harm’ simply to jump on this fad to bring in revenue,” Dr. Spratt said.
Evidence-Based or Oversold?
Focal therapy gained a foothold in the United Kingdom well before the United States.
Hashim Ahmed, FRCS, urology chair at Imperial College London, has used focal therapy for 15 years, treated over 1000 patients, and taught dozens of surgeons how to use the leading focal therapies — focal cryoablation, in which surgeons use a needle-thin probe to target, freeze, and kill prostate tumors, as well as high-intensity focused ultrasound, which uses sound wave energy to superheat and kill tumors.
“Certainly, in the United Kingdom, focal therapy has been prime time in a number of centers for a number of years,” Dr. Ahmed said.
In the United States, focal therapy has become an attractive option for men with prostate cancer who want to avoid radiation or radical prostatectomy but don’t feel comfortable simply monitoring their disease with active surveillance. Experts from specialized focal therapy centers touting the promise of this “innovative technique” predict its routine use in the next few years.
But the excitement surrounding the use of focal therapy in prostate cancer has outpaced broader acceptance.
In 2015, the FDA approved high-intensity focused ultrasound to treat prostatic disease, but not prostate cancer specifically. Although the approval language “means that companies cannot advertise that their devices can be used for prostate cancer,” physicians can still determine how to use the technology, which includes treating prostate cancer, Dr. Ahmed said.
The evidence is starting to catch up to the demand. The latest research suggests that the partial-gland techniques may stand up well to radical prostatectomy.
A 2022 prospective database study comparing radical prostatectomies to focal therapy — mostly high-intensity focused ultrasound — in more than 800 men found similar rates of failure-free survival in the two groups at the 8-year follow-up. A 2019 registry study found that failure-free survival at 3 years was just over 90% in high and intermediate-risk patients receiving focal cryotherapy, with the rate rising to about 93% for the intermediate-risk group. And a 2018 prospective study of 625 patients with intermediate or high-risk prostate cancer who underwent high-intensity focused ultrasound had 5-year metastasis-free survival of 98% and overall survival rates of 100%.
One of the biggest draws of focal therapy vs more aggressive treatments is the “massive differences in side-effect profiles,” said Dr. Ahmed.
In a 2021 meta-analysis, researchers found that 6 months after high-intensity focused ultrasound, 98% of patients remained continent and 80% retained erectile function, while erectile dysfunction can occur in 30% to as many as 85% of patients following prostatectomy or radiotherapy and urinary incontinence can occur in as many as 40% of patients.
Despite these potential advantages of focal therapy, the long-term efficacy of the techniques remains uncertain.
A recent study from a team at MSK, for instance, reported that 40% of men with intermediate (grade 2) or high-risk (grade 3) disease had residual cancer following MRI-guided focused ultrasound. A 2020 prospective registry study found that almost 20% of patients undergoing high-intensity focal ultrasound required a second round following a recurrence.
Dr. Spratt worries that patients who recur after focal therapy may go on to receive a second round — often offered at half price — and will still ultimately need surgery or radiation therapy later. By that point, however, patients may have spent as much as $45,000 — ie, $30,000 on the initial and another $15,000 on the follow-up procedure.
When patients see Dr. Spratt after a recurrence, he informs them that their side effects will be worse if he gives them radiation or surgery now vs if he had given them curative therapy upfront. “But this is what we’re left with,” he tells them.
Another big concern in the field is “the quality of data for focal therapy is overwhelmingly poor,” said Jonathan Shoag, MD, a urologic oncologist at University Hospitals and an associate professor of urology at Case Western Reserve University School of Medicine in Cleveland. “Essentially, the bulk of the data is from single-institution retrospective series without defined follow-up protocols or endpoints.”
The American Urological Association (AUA) has even cautioned experts and patients about the lack of high-quality data comparing focal therapy techniques to radiation therapy, surgery, and active surveillance. According to the AUA, focal options should only be considered in intermediate-risk prostate cancer in a clinical trial setting.
“The lack of randomized clinical trials poses a major stumbling block for the field,” said Dr. Ahmed.
Although randomized trials would be ideal, the results would take many years to mature, and growing patient demand for these less invasive focal procedures has made randomized trials difficult to complete, explained Arvin George, MD, associate professor at Johns Hopkins School of Medicine in Baltimore. Several randomized trials attempted in Norway and the United Kingdom, for instance, fell apart when patients refused to be randomized between focal and radical therapy, Dr. George said.
Focal therapy is now in the same position that active surveillance was a few years ago, according to Dr. George.
“We are hearing the same concerns about focal therapy now as we did about active surveillance,” he said. The initial evidence supporting active surveillance largely came from real-world experience and retrospective studies. The randomized data came later, and skeptics of active surveillance “were proven wrong,” he added.
But Dr. Shoag has a different take on the trajectory of focal therapy research and care in the United States.
“I think there’s this emerging kind of tragedy happening in our field now, where you have even academic institutions offering focal therapy to patients off-trial with essentially no data to suggest it is oncologically effective,” Dr. Shoag said.
William Catalona, MD, Northwestern University Feinberg School of Medicine, Chicago, agreed, noting that too many low-risk patients are undergoing focal treatment who should be on active surveillance. “Many men are attracted to focal because they just are uncomfortable having a cancer in their body that’s not treated,” Dr. Catalona said. But “giving these patients focal therapy is really overtreatment.”
Patients with higher-risk disease who want to avoid aggressive treatment are also being lured into focal without guidelines or clear evidence to back up that option, Dr. Catalona explained.
Although it’s not clear how many men in the United States are receiving focal therapy who shouldn’t, even proponents of focal therapy, like George, have expressed concern.
Dr. George agreed that focal therapy marketing geared towards patients is drawing in some men who are not good candidates for these techniques, and feels there’s not enough objective material from medical societies or academic centers giving patients a realistic picture of focal therapy.
“There is concern that patients may be receiving biased information,” Dr. George said, adding that it’s ultimately up to the physician to reconcile the best available evidence, understand the outcomes, and discuss these options with the patient to guide them to what’s best.
At the end of the day, Dr. Spratt said, physicians giving focal therapy off a clinical trial need to pause and ask themselves “why are they giving a treatment that remains investigational by payers, not recommended by any major guideline, and that lacks any randomized evidence?”
Mr. LaFrate does not regret his decision to forgo focal therapy in 2013. He has been on active surveillance for about a decade now.
Following an MRI in 2022, Mr. LaFrate’s radiology report found that “clinically significant cancer is very unlikely to be present.”
Still, his PSA has risen two points in the past year to 14. His current urologist feels that the PSA is going up because there’s cancer present and is suggesting focal therapy for Mr. LaFrate.
Mr. LaFrate, who has prostate enlargement issues, remains skeptical of focal therapy and is still resisting the sales pitch.
“My doctor is not aggressively pushing it. He’s just giving me that as one of my options,” he said. “I just have a hunch I don’t need it at this point.”
A version of this article appeared on Medscape.com.
In 2013, a prostate-specific antigen (PSA) blood test revealed that Richard LaFrate’s levels had jumped.
Previously in a normal range, his PSA was now above 6 ng/mL, indicating an elevated likelihood for prostate cancer. The jazz guitarist from Leesburg, Florida, then 70 years old, underwent a biopsy, which found two Gleason 6 lesions.
Mr. LaFrate had low-risk prostate cancer.
Guidelines now recommend active surveillance for patients like Mr. LaFrate, who have low-risk disease. This strategy would mean monitoring the cancer until LaFrate required treatment, with the upside being he might never need therapy.
Mr. LaFrate’s urologist, however, was pushing whole gland surgery — an invasive and unnecessary procedure given his diagnosis and age.
Mr. LaFrate decided to look for another doctor. He filled out a form online that pointed him to a new urologist who offered him one option: An investigational procedure known as high-intensity focused ultrasound.
At the time, high-intensity focused ultrasound — a form of focal therapy — was being studied in the United States to treat men with low or intermediate-risk prostate cancer, but it was still relatively early days.
Mr. LaFrate’s urologist asked him to pay $25,000 out of pocket to undergo the focal procedure at a clinic in the Bahamas. He refused and, ultimately, landed on active surveillance as the best strategy to manage for his low-risk disease.
That urologist was “a shyster in my opinion,” Mr. LaFrate said.
— Gleason 3+4 (grade group 2) tumors — as an alternative to invasive surgery and active surveillance. Prestigious medical centers, such as Cleveland Clinic, Mayo Clinic, Memorial Sloan Kettering, UCLA, and the University of Chicago, routinely offer focal therapy.
But use of the techniques remains controversial and costly.
As the Cleveland Clinic’s website acknowledges, although “the use of focal therapy for localized prostate cancer appears to be a promising development in a number of ways, it is still considered investigational and not yet part of standard therapy.” Major caveats to focal therapy include unknown long-term effectiveness, the possibility of leaving behind untreated cancer, and higher overall costs.
No major national guidelines endorse the use of focal therapy, unless offered in a research or clinical trial setting. Insurance companies, such as Aetna, Blue Cross Blue Shield, and United, also consider focal therapy for prostate cancer investigational and don’t cover it.
Without a stamp of approval from guideline bodies and insurance companies, patients, like Mr. LaFrate, remain vulnerable to the high out-of-pocket costs for these focal techniques.
“Almost every place charges $15,000-$30,000 in cash,” said Daniel Spratt, MD, radiation oncology chair at University Hospitals Seidman Cancer Center and Case Western Reserve University in Cleveland.
Dr. Spratt has seen hundreds of patients after focal therapy, some from prominent centers, who have emptied their bank accounts to undergo treatment with the promise of great results and ultimately felt misled when the cancer has recurred.
“It pains me that there are doctors willing to ignore the Hippocratic oath of ‘Do No Harm’ simply to jump on this fad to bring in revenue,” Dr. Spratt said.
Evidence-Based or Oversold?
Focal therapy gained a foothold in the United Kingdom well before the United States.
Hashim Ahmed, FRCS, urology chair at Imperial College London, has used focal therapy for 15 years, treated over 1000 patients, and taught dozens of surgeons how to use the leading focal therapies — focal cryoablation, in which surgeons use a needle-thin probe to target, freeze, and kill prostate tumors, as well as high-intensity focused ultrasound, which uses sound wave energy to superheat and kill tumors.
“Certainly, in the United Kingdom, focal therapy has been prime time in a number of centers for a number of years,” Dr. Ahmed said.
In the United States, focal therapy has become an attractive option for men with prostate cancer who want to avoid radiation or radical prostatectomy but don’t feel comfortable simply monitoring their disease with active surveillance. Experts from specialized focal therapy centers touting the promise of this “innovative technique” predict its routine use in the next few years.
But the excitement surrounding the use of focal therapy in prostate cancer has outpaced broader acceptance.
In 2015, the FDA approved high-intensity focused ultrasound to treat prostatic disease, but not prostate cancer specifically. Although the approval language “means that companies cannot advertise that their devices can be used for prostate cancer,” physicians can still determine how to use the technology, which includes treating prostate cancer, Dr. Ahmed said.
The evidence is starting to catch up to the demand. The latest research suggests that the partial-gland techniques may stand up well to radical prostatectomy.
A 2022 prospective database study comparing radical prostatectomies to focal therapy — mostly high-intensity focused ultrasound — in more than 800 men found similar rates of failure-free survival in the two groups at the 8-year follow-up. A 2019 registry study found that failure-free survival at 3 years was just over 90% in high and intermediate-risk patients receiving focal cryotherapy, with the rate rising to about 93% for the intermediate-risk group. And a 2018 prospective study of 625 patients with intermediate or high-risk prostate cancer who underwent high-intensity focused ultrasound had 5-year metastasis-free survival of 98% and overall survival rates of 100%.
One of the biggest draws of focal therapy vs more aggressive treatments is the “massive differences in side-effect profiles,” said Dr. Ahmed.
In a 2021 meta-analysis, researchers found that 6 months after high-intensity focused ultrasound, 98% of patients remained continent and 80% retained erectile function, while erectile dysfunction can occur in 30% to as many as 85% of patients following prostatectomy or radiotherapy and urinary incontinence can occur in as many as 40% of patients.
Despite these potential advantages of focal therapy, the long-term efficacy of the techniques remains uncertain.
A recent study from a team at MSK, for instance, reported that 40% of men with intermediate (grade 2) or high-risk (grade 3) disease had residual cancer following MRI-guided focused ultrasound. A 2020 prospective registry study found that almost 20% of patients undergoing high-intensity focal ultrasound required a second round following a recurrence.
Dr. Spratt worries that patients who recur after focal therapy may go on to receive a second round — often offered at half price — and will still ultimately need surgery or radiation therapy later. By that point, however, patients may have spent as much as $45,000 — ie, $30,000 on the initial and another $15,000 on the follow-up procedure.
When patients see Dr. Spratt after a recurrence, he informs them that their side effects will be worse if he gives them radiation or surgery now vs if he had given them curative therapy upfront. “But this is what we’re left with,” he tells them.
Another big concern in the field is “the quality of data for focal therapy is overwhelmingly poor,” said Jonathan Shoag, MD, a urologic oncologist at University Hospitals and an associate professor of urology at Case Western Reserve University School of Medicine in Cleveland. “Essentially, the bulk of the data is from single-institution retrospective series without defined follow-up protocols or endpoints.”
The American Urological Association (AUA) has even cautioned experts and patients about the lack of high-quality data comparing focal therapy techniques to radiation therapy, surgery, and active surveillance. According to the AUA, focal options should only be considered in intermediate-risk prostate cancer in a clinical trial setting.
“The lack of randomized clinical trials poses a major stumbling block for the field,” said Dr. Ahmed.
Although randomized trials would be ideal, the results would take many years to mature, and growing patient demand for these less invasive focal procedures has made randomized trials difficult to complete, explained Arvin George, MD, associate professor at Johns Hopkins School of Medicine in Baltimore. Several randomized trials attempted in Norway and the United Kingdom, for instance, fell apart when patients refused to be randomized between focal and radical therapy, Dr. George said.
Focal therapy is now in the same position that active surveillance was a few years ago, according to Dr. George.
“We are hearing the same concerns about focal therapy now as we did about active surveillance,” he said. The initial evidence supporting active surveillance largely came from real-world experience and retrospective studies. The randomized data came later, and skeptics of active surveillance “were proven wrong,” he added.
But Dr. Shoag has a different take on the trajectory of focal therapy research and care in the United States.
“I think there’s this emerging kind of tragedy happening in our field now, where you have even academic institutions offering focal therapy to patients off-trial with essentially no data to suggest it is oncologically effective,” Dr. Shoag said.
William Catalona, MD, Northwestern University Feinberg School of Medicine, Chicago, agreed, noting that too many low-risk patients are undergoing focal treatment who should be on active surveillance. “Many men are attracted to focal because they just are uncomfortable having a cancer in their body that’s not treated,” Dr. Catalona said. But “giving these patients focal therapy is really overtreatment.”
Patients with higher-risk disease who want to avoid aggressive treatment are also being lured into focal without guidelines or clear evidence to back up that option, Dr. Catalona explained.
Although it’s not clear how many men in the United States are receiving focal therapy who shouldn’t, even proponents of focal therapy, like George, have expressed concern.
Dr. George agreed that focal therapy marketing geared towards patients is drawing in some men who are not good candidates for these techniques, and feels there’s not enough objective material from medical societies or academic centers giving patients a realistic picture of focal therapy.
“There is concern that patients may be receiving biased information,” Dr. George said, adding that it’s ultimately up to the physician to reconcile the best available evidence, understand the outcomes, and discuss these options with the patient to guide them to what’s best.
At the end of the day, Dr. Spratt said, physicians giving focal therapy off a clinical trial need to pause and ask themselves “why are they giving a treatment that remains investigational by payers, not recommended by any major guideline, and that lacks any randomized evidence?”
Mr. LaFrate does not regret his decision to forgo focal therapy in 2013. He has been on active surveillance for about a decade now.
Following an MRI in 2022, Mr. LaFrate’s radiology report found that “clinically significant cancer is very unlikely to be present.”
Still, his PSA has risen two points in the past year to 14. His current urologist feels that the PSA is going up because there’s cancer present and is suggesting focal therapy for Mr. LaFrate.
Mr. LaFrate, who has prostate enlargement issues, remains skeptical of focal therapy and is still resisting the sales pitch.
“My doctor is not aggressively pushing it. He’s just giving me that as one of my options,” he said. “I just have a hunch I don’t need it at this point.”
A version of this article appeared on Medscape.com.
Plant-Based Diet a Boon for Men With Prostate Cancer
, new research showed.
The findings, published on February 13, 2024, in the journal Cancer, bolster previous research showing plant-based diets can reduce the risk for recurrence and improve survivorship in men with prostate cancer.
“The current study shows for the first time an association between eating more plant-based food with better scores for quality of life among patients diagnosed with prostate cancer,” Stacy Loeb, MD, a urologist in the departments of Urology and Population Health at NYU Langone Health, in New York City, who led the research.
For the new study, Dr. Loeb and her colleagues looked at data from more than 3500 men with prostate cancer in the Health Professionals Follow-Up Study, an ongoing investigation begun in 1986 and sponsored by Harvard T.H. Chan School of Public Health. The dataset included more than 50,000 male dentists, pharmacists, optometrists, osteopaths, podiatrists, and veterinarians.
The median age of prostate cancer diagnosis was 68 years; 48% of patients underwent radical prostatectomy and 35% had radiation as primary therapy. None of the patients were known to have had metastatic disease.
Men in the study answered a questionnaire every 4 years about the kinds of foods they ate and in what proportions. Another survey, administered every 2 years, assessed the frequency of incontinence, difficulties maintaining an erection, and problems with bowels, energy, and mood, among many other health concerns.
Dr. Loeb and her colleagues sorted patients into quintiles based on the proportion of plant vs animal foods the men said they eat. The authors found those who consumed the most plant-based foods scored 8%-11% better in measures of sexual function than the group that consumed the least of these products.
These men also reported up to 14% better scores for urinary health, with fewer instances of incontinence, obstruction, and irritation, and up to 13% better scores in hormonal health, marked by symptoms like low energy, depression, and hot flashes.
Justin Gregg, MD, a urology researcher at the University of Texas MD Anderson Cancer Center, in Houston, Texas, whose research has found the Mediterranean diet can slow tumor progression among men with localized prostate cancer on active surveillance, called the results “not entirely surprising, as prior studies have shown associations between plant-based diet and outcomes like erectile function among men who do not have prostate cancer.”
But Kenneth Jacobsohn, MD, professor of urology and director of lifestyle medicine at the Medical College of Wisconsin, in Milwaukee, said the new findings help establish “the positive role of diet quality and plant-based diets, specifically on quality of life after prostate cancer diagnosis and treatment for men with nonmetastatic prostate cancer.”
Dr. Jacobsohn said the study was limited by its retrospective nature and the manner of the dietary assessment.
“As the authors point out, a plant-based diet may be helpful, though it’s important to keep in mind the strong data for its protective effect in terms of cardiovascular disease risk, which is very important for men who have a history of prostate cancer as many will die of cardiovascular disease,” Dr. Gregg added.
Dr. Loeb, Dr. Gregg, and Dr. Jacobsohn reported no conflicts of interest. Some of the study authors reported a variety of potential conflicts.
A version of this article appeared on Medscape.com .
, new research showed.
The findings, published on February 13, 2024, in the journal Cancer, bolster previous research showing plant-based diets can reduce the risk for recurrence and improve survivorship in men with prostate cancer.
“The current study shows for the first time an association between eating more plant-based food with better scores for quality of life among patients diagnosed with prostate cancer,” Stacy Loeb, MD, a urologist in the departments of Urology and Population Health at NYU Langone Health, in New York City, who led the research.
For the new study, Dr. Loeb and her colleagues looked at data from more than 3500 men with prostate cancer in the Health Professionals Follow-Up Study, an ongoing investigation begun in 1986 and sponsored by Harvard T.H. Chan School of Public Health. The dataset included more than 50,000 male dentists, pharmacists, optometrists, osteopaths, podiatrists, and veterinarians.
The median age of prostate cancer diagnosis was 68 years; 48% of patients underwent radical prostatectomy and 35% had radiation as primary therapy. None of the patients were known to have had metastatic disease.
Men in the study answered a questionnaire every 4 years about the kinds of foods they ate and in what proportions. Another survey, administered every 2 years, assessed the frequency of incontinence, difficulties maintaining an erection, and problems with bowels, energy, and mood, among many other health concerns.
Dr. Loeb and her colleagues sorted patients into quintiles based on the proportion of plant vs animal foods the men said they eat. The authors found those who consumed the most plant-based foods scored 8%-11% better in measures of sexual function than the group that consumed the least of these products.
These men also reported up to 14% better scores for urinary health, with fewer instances of incontinence, obstruction, and irritation, and up to 13% better scores in hormonal health, marked by symptoms like low energy, depression, and hot flashes.
Justin Gregg, MD, a urology researcher at the University of Texas MD Anderson Cancer Center, in Houston, Texas, whose research has found the Mediterranean diet can slow tumor progression among men with localized prostate cancer on active surveillance, called the results “not entirely surprising, as prior studies have shown associations between plant-based diet and outcomes like erectile function among men who do not have prostate cancer.”
But Kenneth Jacobsohn, MD, professor of urology and director of lifestyle medicine at the Medical College of Wisconsin, in Milwaukee, said the new findings help establish “the positive role of diet quality and plant-based diets, specifically on quality of life after prostate cancer diagnosis and treatment for men with nonmetastatic prostate cancer.”
Dr. Jacobsohn said the study was limited by its retrospective nature and the manner of the dietary assessment.
“As the authors point out, a plant-based diet may be helpful, though it’s important to keep in mind the strong data for its protective effect in terms of cardiovascular disease risk, which is very important for men who have a history of prostate cancer as many will die of cardiovascular disease,” Dr. Gregg added.
Dr. Loeb, Dr. Gregg, and Dr. Jacobsohn reported no conflicts of interest. Some of the study authors reported a variety of potential conflicts.
A version of this article appeared on Medscape.com .
, new research showed.
The findings, published on February 13, 2024, in the journal Cancer, bolster previous research showing plant-based diets can reduce the risk for recurrence and improve survivorship in men with prostate cancer.
“The current study shows for the first time an association between eating more plant-based food with better scores for quality of life among patients diagnosed with prostate cancer,” Stacy Loeb, MD, a urologist in the departments of Urology and Population Health at NYU Langone Health, in New York City, who led the research.
For the new study, Dr. Loeb and her colleagues looked at data from more than 3500 men with prostate cancer in the Health Professionals Follow-Up Study, an ongoing investigation begun in 1986 and sponsored by Harvard T.H. Chan School of Public Health. The dataset included more than 50,000 male dentists, pharmacists, optometrists, osteopaths, podiatrists, and veterinarians.
The median age of prostate cancer diagnosis was 68 years; 48% of patients underwent radical prostatectomy and 35% had radiation as primary therapy. None of the patients were known to have had metastatic disease.
Men in the study answered a questionnaire every 4 years about the kinds of foods they ate and in what proportions. Another survey, administered every 2 years, assessed the frequency of incontinence, difficulties maintaining an erection, and problems with bowels, energy, and mood, among many other health concerns.
Dr. Loeb and her colleagues sorted patients into quintiles based on the proportion of plant vs animal foods the men said they eat. The authors found those who consumed the most plant-based foods scored 8%-11% better in measures of sexual function than the group that consumed the least of these products.
These men also reported up to 14% better scores for urinary health, with fewer instances of incontinence, obstruction, and irritation, and up to 13% better scores in hormonal health, marked by symptoms like low energy, depression, and hot flashes.
Justin Gregg, MD, a urology researcher at the University of Texas MD Anderson Cancer Center, in Houston, Texas, whose research has found the Mediterranean diet can slow tumor progression among men with localized prostate cancer on active surveillance, called the results “not entirely surprising, as prior studies have shown associations between plant-based diet and outcomes like erectile function among men who do not have prostate cancer.”
But Kenneth Jacobsohn, MD, professor of urology and director of lifestyle medicine at the Medical College of Wisconsin, in Milwaukee, said the new findings help establish “the positive role of diet quality and plant-based diets, specifically on quality of life after prostate cancer diagnosis and treatment for men with nonmetastatic prostate cancer.”
Dr. Jacobsohn said the study was limited by its retrospective nature and the manner of the dietary assessment.
“As the authors point out, a plant-based diet may be helpful, though it’s important to keep in mind the strong data for its protective effect in terms of cardiovascular disease risk, which is very important for men who have a history of prostate cancer as many will die of cardiovascular disease,” Dr. Gregg added.
Dr. Loeb, Dr. Gregg, and Dr. Jacobsohn reported no conflicts of interest. Some of the study authors reported a variety of potential conflicts.
A version of this article appeared on Medscape.com .